This Policy Exchange report marks an important contribution to the growing
body of evidence demonstrating that urgent attention needs to be paid to the
ways children are being impacted by gender identity beliefs. Safeguarding
principles are foundational to the functioning of a responsible society, and there
is absolutely no reason why schools should ever compromise these principles.
Children deserve to explore the ways they feel about themselves and the world
in ways which do not harm them. Every issue concerning children should be
viewed through a safeguarding lens, and there is no reason why gender distress
should be any different.

Safeguarding principles are fundamental to a responsible society – and all
teachers know that. Yet this report by Policy Exchange demonstrates the
incompatibility between current practice for gender distressed children and
well-established and universally accepted safeguarding principles. The report’s
recommendations must be implemented - we cannot compromise child wellbeing
in favour of gender identity beliefs. Given what has happened within clinical
settings with Dr Cass’ damning report and the subsequent closure of GIDS,
Government must issue clearer guidance to schools so that no school facilitates
affirmative practice. Children deserve to be kept safe and action is now urgent.

“Safeguarding should always be a prime concern for schools and it is deeply
concerning that this Policy Exchange report suggests that this is being
undermined in some cases. I support high quality Relationships, Sex and Health
Education & building confidence to deliver this well should be a priority for the
Government. What should never be happening is contested theories being taught
as fact something that goes against the spirit and the letter of the Department’s
own political impartiality guidance and my committee have been pressing the
Government to update its guidance on RSHE to make sure this isn’t the case.
Parents always have the right to know about the materials being used to teach
their children and to have a say in decisions being taken about their welfare.
“Parents need the reassurance that they will be properly informed and supported
to safeguard the best interests of their children and should never have to worry
about contested ideology being imposed or medical decisions being taken without
their knowledge. I welcome the fact that the report acknowledges that the vast
majority of teachers, schools and parents want to do the right thing for children
and keep them safe. Government policy and guidance needs to support this.”

This is an outstanding report from Policy Exchange and offers an invaluable
and timely insight into the shocking extent of safeguarding failures in many
British schools. The protection of children from political indoctrination is
foundational to democratic society, and yet this report shows that we are
currently failing to protect a whole generation of children from the destructive
effects of extreme gender ideology.
For years, parents who have raised safeguarding concerns to both schools
and the Department for Education have been ignored, disbelieved or labelled as
‘bigots’. This report is a vindication of their concerns and a resounding call to
action for Government and school leaders. Biological sex is immutable and the
sex-based protections that are the hallmark of all civilised societies must apply
to children in our schools.

This report by Policy Exchange disproves the thesis that extreme political
ideology is happening in ‘just a few schools’. Rather, the research published
within this paper demonstrates that gender ideology is built into the core values
ofa number of schools. The fact that only 28% of schools are reliably informing
parents as soon as a child discloses feelings of gender distress suggests schools are actively presuming parents to be a risk to the welfare of their children.
The erosion of single-sex boundaries – at least 28% of schools are not
maintaining single-sex toilets – should concern us all. This report lays bare the
stark reality that some schools are routinely placing contested gender identity
beliefs ahead of child wellbeing. We cannot erase the notion of biological sex.
As a lawmaker, and a father of two daughters, I call on the Government to
act.

Parents place overwhelming trust in their child’s school to ensure they are
kept safe from harm. Policy Exchange reveals a systemic safeguarding blind
spot when it comes to gender-distressed children and their peers. There is no
reason why gender distress should be exempt from safeguarding standards that
have been enshrined in law for decades. The report also shows how radical and
unscientific beliefs have become embedded into the heart of the school system,
often, but not only, via Relationship and Sex Education lessons.
This is in contravention of the Education Act which forbids the partisan
teaching of ideology in schools. But it is also starting to undermine parental
faith in our school system – note, for example, the small but steady increase in
home schooling. However, at the same time, there is no doubt that schools are
being asked to take on more and more of society’s transmission of its moral and
cultural values, just as these are being increasingly contested. I therefore endorse
all of Policy Exchange’s recommendations, but two in particular.
First, it is time to stand back and commission an independent review that
involves parents, teachers, faith and community groups that is tasked to look
with fresh eyes at the school role in transmitting our society’s core values.
Second, because we will never perfect this school role, nor how it can be guided
by governments, we must embed an inalienable right for parents to view and
engage with all school curriculum materials. This is the best mechanism to
both safeguard our children and to help schools navigate their discussion around
the complex social issues arising in our modern world.

How is it that (under the radar) schools started teaching children that biological sex was somehow unimportant, or even a cultural attribute? Childhood is just when we all start emerging as sexual adults – often a confusing and troublesome time when support, guidance, and safeguarding may be needed from family and school. Importantly, children – especially girls – need privacy, protection and opportunities, in the changing room as well as on the sports field. The findings of this report suggest that many are being let down. So this is a call to arms – for schools, the relevant authorities and parents – to place children’s interests at the centre of our education provision.



Authors

Content
+
-
- 7.1 To what extent are schools involving parents?
- 7.2 To what extent are schools involving safeguarding or medical professionals?
- 7.3 To what extent are schools operating policies of gender self-identification?
- 7.4 How are other children impacted by schools’ approaches to gender-distressed children?
- 7.5 What are schools teaching on sex and gender?
- 7.6 What sorts of external agencies are schools using?
-
Foreword
Rosie Duffield MP,
Member of Parliament for Canterbury, Whitstable and the Villages
Co-Patron of Policy Exchange’s Biology Matters Project
Children deserve to be children. Parents place profound trust in schools to ensure their children are able to learn and flourish, and most importantly – be kept safe from harm. Safeguarding principles are designed to facilitate this. So why are so many schools breaking them in order to pursue a highly contested set of beliefs about gender identity?
The number of children presenting with gender distress has increased dramatically over the last five years, in part because of extreme ideological ideas that are being promoted in schools. Children as young as five are being encouraged to question their gender identity, or being taught they have been ‘born in the wrong body’ if they do not conform to regressive gender stereotypes. In this report, Policy Exchange reveals that a generation of children are being let down, because well-established safeguarding standards are being compromised.
There has been a determined attempt to dismiss these concerns, by suggesting that such practice is only happening in a few secondary schools. There has been an unwillingness to confront the truth. Policy Exchange exposes the reality that this ideology is widespread across secondary schools. This Government has failed children by allowing partisan beliefs to become entrenched within the education system. Meanwhile, the Opposition has failed to pull them up on it.
Schools – who take on immense responsibility for educating our children – are facilitating medical interventions, with the impossibility of knowing whether this is in their best interests. New Policy Exchange research reveals that only 28 per cent of secondary schools are reliably informing parents of their children’s’ gender distress. Those who query whether affirmation is right for their child are side-lined. Four in ten secondary schools operate policies of gender-self-ID. At least 19 per cent of secondary schools are failing to maintain single-sex changing rooms, leaving vulnerable adolescent girls forced to share their spaces with males.
Despite their legal obligations to be politically impartial, beliefs about gender identity have become embedded within the curriculum as though they are facts. With so many schools teaching children that potentially transient feelings about their gender are more determinative of their identity than their chromosomal DNA, it is unsurprising that so many present with distress at their developing bodies. The argument that these lessons are only happening in a small number of schools is disproved by the research presented in this report. The endorsement of charities that promote these partisan beliefs by the Department of Education itself demonstrates this is not a case of ‘one bad apple’. Rather, it appears the system is rotten to the core.
There is a growing body of evidence demonstrating that the affirmative approach to gender distressed children is not a one-size-fits-all solution. The NHS commissioned review by Dr Hilary Cass and its damning findings about the failures of the Tavistock against gender-distressed children is testament to this. While it is right that the clinical failures suffered by countless children with gender distress has been rightly exposed, these failures are being repeated in the school system. Those in authority – who should be putting children’s’ best interests first – have been asleep at the wheel. Thousands of children are being harmed because of their failure to stand up to the radical beliefs being pushed by campaigners.
The safeguarding of children is fundamental to a civilised society. Policy Exchange here demonstrates there to be a systemic failure in the school system, caused by an ill-considered embrace of gender ideology. There has been little consideration of the consequences on the children our schools are there to protect, and it they who are paying the price. We must end this reckless experiment now.
Next chapterExecutive Summary
Schools take on immense responsibility for equipping children with the knowledge they need to thrive as adults. It goes well beyond the planning, preparation and delivery of lessons and the focus on a child’s academic development. This report starts from the premise that teachers, parents and carers are united in wanting the best for children. However, over the last decade, a set of contested beliefs have become embedded within many schools, operating in a way that compromises safeguarding principles and risks jeopardising the wellbeing of children.
A fundamental component of how schools discharge their duties is through safeguarding. Safeguarding refers to a range of measures that must be met to ensure children are healthy, safe, and able to flourish.1HM Government, Working Together to Safeguard Children, A guide to inter-agency working to safeguard and promote the welfare of children, July 2019, pg.6. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/942454/Working_together_to_safeguard_children_inter_agency_guidance.pdf These principles are well-established, enshrined in law, and universally understood to be instrumental to the functioning of a responsible society. Safeguarding principles include maintaining parental involvement in their child’s life, ensuring that when a child discloses a potential concern it is shared with the appropriate partners immediately, and collaborating with local services in order to ensure that relevant professionals can respond to concerns as soon as possible.
Our research reveals there to be a safeguarding blind spot when it comes to the issue of sex and gender. Safeguarding principles are being routinely disregarded in many secondary schools, which are neglecting their safeguarding responsibilities and principles in favour of a set of contested beliefs, in ways that risk jeopardising child wellbeing and safety. In doing so, schools are compromising both the law and statutory safeguarding guidance. Many schools are also disregarding published guidance in the teaching of the Relationships, Sex and Health Education (RSHE) teaching curriculum, and their legal requirements to remain politically impartial. This report focuses on the conflict between the application of gender identity beliefs in school, and the safeguarding principles they are required to adhere to.
By uncritically accepting contested beliefs on gender identify, as well as adopting affirmative practice, which involves affirming a child’s belief that they are the opposite gender to their sex, schools are failing to consider their safeguarding duties – not just to gender-distressed children – but to their peers as well. We have uncovered numerous cases of schools acting in complete disregard of standard safeguarding procedures, including by not informing parents – without good reason – in major life decisions by their child, promising confidentiality to a child about certain matters, or allowing children to make significant, potentially irreversible medical decisions without involving either parents or relevant professionals.2This report will use parents henceforth to mean both parents and guardians/carers.
Encouraged by external agencies, schools have been adopting these practices in an attempt to deal with the rising numbers of children presenting with gender distress. Consequently, established laws and safeguarding norms are being disregarded, as teachers facilitating the social transition of children with the impossibility of knowing whether this is in a child’s best interests. Schools often overlook how affirmative practice affects their safeguarding duties towards other children, who are required to compromise their own rights to single-sex spaces as a condition of receiving their education.
External agencies also have considerable influence in embedding gender identity beliefs within the RSHE curriculum. Schools are teaching beliefs about gender identity as though they are facts, often presenting the immutable and biological reality of sex as less important than a person’s ineffable feelings about themselves. Many of the cultural and social attributes associated with genders are based on regressive sex stereotypes.
There is a misconception that such practice is hypothetical, or only happening in an isolated number of secondary schools. This report disproves that thesis. Following extensive research in which Policy Exchange sent Freedom of Information (FOI) requests to a random selection of over 300 maintained secondary schools and academies in England, a substantial percentage of schools are disregarding basic safeguarding protocol regarding gender-distressed children and their peers:
- Only 28 per cent of secondary schools are reliably informing parents as soon as a child discloses feelings of gender distress.
- 33 per cent of secondary schools did not say they would inform their Designated Safeguarding Lead or a medical practitioner when a child discloses gender distress.
- Four in ten secondary schools operate policies of gender self-identification.
- At least 28 per cent of secondary schools are not maintaining single sex toilets, and 19 per cent are not maintaining single-sex changing rooms. 60 per cent of secondary schools are allowing children to participate in sports of the opposite sex.
- 69 per cent of secondary schools are requiring other children to affirm a gender-distressed child’s new identity.
- With regard to what secondary schools are teaching in Relationships, Sex and Health Education (RSHE):
- 72 per cent of schools are teaching that people have a gender identity that may be different from their biological sex
- 25 per cent are teaching that some people or children ‘may be born in the wrong body.’
- 30 per cent are teaching pupils that a person who self-identifies as a man or a woman should be treated as a man or woman in all circumstances, even if this does not match their biological sex.
Key to understanding why so many schools are compromising their safeguarding standards on this issue requires exploring the wider climate within the UK’s education system on sex and gender. Over the last decade, external agencies with partisan (and sometimes overtly political) aims have received large amounts of government funding and, accordingly, have gained influence within the education sector. They have used this influence to embed contested gender identity beliefs within schools. Such organisations have, perhaps unwittingly, encouraged schools to compromise safeguarding principles and the rights of other pupils under the guise of noble aims such as equality, anti-bullying, and LGBT inclusion.
Over the last year, clinical provision for gender distressed children has come under scrutiny. An NHS commissioned report published by Dr Hilary Cass found serious failings with the Gender Identity Development Service (GIDS), which is responsible for the clinical provision of gender-distressed children. Dr Cass found there to be a lack of clinical agreement at “primary, secondary and specialist level” about the nature of affirmative practice as a solution to gender distress.3The Cass Review, Independent review of gender identity services for children and young people: Interim report, February 2022, pg.16. https://cass.independent-review.uk/publications/interim-report/ Given such treatment is still contested in clinical settings, it is entirely inappropriate that large numbers of schools are adopting this approach.
For a very small number of children, affirmation may be the appropriate course of action, after considerable clinical expertise has deemed so. However, gender distress is a complex condition that requires thoughtful judgement. Teachers do not have the authority to makes these judgements, and school is not the setting in which these complexities can be resolved. Safeguarding principles protect both children and the staff who look after them. Within society, schools play an indispensable part in children’s lives: in enabling them to learn and in keeping them safe. Decisions made in the absence of parental consent and democratic consensus as the result of contested political ideas must not interfere with this essential role.
Recommendations
|
1. Introduction
The number of children presenting with gender distress has escalated over the past decade, but particularly so in the last five years. The recency and scale of this phenomenon has resulted in a general failure to assess whether approaches to children experiencing gender distress align with wider mandatory safeguarding strategies applicable to all organisations and functions relating to children. The government’s definition of safeguarding encompasses a holistic range of measures that must be met to ensure children are safe, healthy and able to flourish.4WTTSC, pg. 6-7. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/942454/Working_together_to_safeguard_children_inter_agency_guidance.pdf
The number of children being referred to the Gender Identity Development Service (GIDS) has risen by over 1600 per cent since 2010, and referral rates among girls are much higher, increasing by 3176 per cent since 2010.5Gender Identity Development Service, Number of Referrals to GIDS. https://gids.nhs.uk/about-us/number-of-referrals/ According to GIDS data published in 2018, 35 per cent of children referred to the service presented with moderate to severe autistic traits.6G. Butler, N. De Graaf, B. Wren et al, Assessment and support of children and adolescents with gender dysphoria, Archives of Disease in Childhood 2018;103:631-636. http://dx.doi.org/10.1136/archdischild-2018-314992 Looked after and adopted children represent significantly higher referrals than the national average (4.9 per cent and 3.8 per cent respectively despite making up only 0.58 per cent of the population).7T. Matthews, V. Holt, S. Sahin et al, Gender Dysphoria in looked-after and adopted young people in a gender identity development service, Clinical Child Psychology and Psychiatry, Volume 24, Issue 1, January 2019. https://journals.sagepub.com/doi/epub/10.1177/1359104518791657. On average, the number of referrals are increasing by 6 per cent every year.8Gender Identity Development Service, Number of Referrals to GIDS.
Gender distress, which is diagnosed in a clinical setting as gender dysphoria, is described by the NHS as “a term that describes a sense of unease that a person may have because of a mismatch between their biological sex and their gender identity.”9NHS, Gender Dysphoria, last reviewed: 28 May 2020. https://www.nhs.uk/conditions/gender-dysphoria/ The NHS states that gender dysphoria is not a mental illness. However, it is a medical condition that can involve treatment. It is included as a health condition in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (DSM-5), which is the principle diagnostic tool for psychiatric disorders within the US, and is considered a worldwide standard.10American Psychiatric Association, What is Gender Dysphoria? https://www.psychiatry.org/patients-families/gender-dysphoria/what-is-gender-dysphoria. It is also included as a health condition within the International Classification of the World Health Organisation (WHO).11World Health Organisation, Gender incongruence and transgender health in the ICD. https://www.who.int/standards/classifications/frequently-asked-questions/gender-incongruence-and-transgender-health-in-the-icd
Public unease at the rising number of children reporting to experience gender distress and/or identifying as transgender is matched with concern about whether the treatment pathway these children are experiencing is adequate. In 2020, the NHS announced that paediatrician Dr Hilary Cass would lead an independent review into gender identity services for children and young people. The Interim Report was published in February 2022, which stated clearly that current provision is not fit for purpose, with services being predominately driven by ‘an affirmative, non-exploratory approach.’12The Cass Review, pg.17. A gender affirmative approach is one that seeks to solve a child’s gender distress by affirming their belief that they are the opposite sex, without exploration of other contributing factors. Social transition is a medical intervention in which a child adopts attributes associated with the opposite sex. This is often considered the first form of treatment advocated for by affirmative practice. Gender transition very often leads to painful and life-changing medical intervention. For a small number of children, gender distress may be resolved through transition. In these circumstances, it is possible that gender affirmation will be the appropriate course of action, if considerable clinical expertise deems it to be so.
Schools have been left to create new policies in order to deal with the influx of children presenting with gender distress, many of which advocate an unquestioning, gender-affirmative approach. This is problematic because the nature of affirmative practice is fundamentally medical. Consequently, well-established laws and safeguarding norms are being substantially jeopardised, with schools unwittingly pushing children onto a pathway of profound and life-altering medical intervention – with the impossibility of knowing whether this is in the child’s best interest.
This problem is further exacerbated by contentious political debates around sex and gender. Over the past decade, external agencies and charities have sought to help schools navigate these issues, sometimes by encouraging them and other public institutions to adopt particular beliefs about gender identity. While ‘sex’ refers to the biological anatomy of male and female, ‘gender’ refers to the cultural and social attributes associated with the sexes. Gender identity beliefs work from the premise that every person has an innate gender identity, based upon these cultural and social attributes, which may or may not match their biological sex. The notion that every person has an innate gender identity is a highly contested belief, unsupported by scientific evidence. Some of these organisations also work towards explicitly political aims, such as lobbying the government to adopt legal sex self-identification, in order to legislate for the belief that gender is more determinative of a person’s identity than their biological sex.
This report will firstly outline the well-established safeguarding norms and standards that schools must adhere to, before explaining guidelines on RSHE teaching about sex and gender. The third chapter will highlight what gender-affirmative care looks like in the UK, before subsequently exploring particular traits and trends in the current caseload of children reporting to experience gender distress. In December 2022, Policy Exchange conducted an FOI research project to assess the extent to which a sample of secondary schools are upholding safeguarding principles on the sex and gender issue. After demonstrating the scale of the problem within schools, this report will highlight exactly why affirmative practice is so problematic. Consequently, it will look at how schools came to be in a situation where such safeguarding breaches have been able to occur, by assessing the wider Department for Education (DfE) approach. Finally, it will offer recommendations as to what can be done next to ensure safeguarding is re-prioritised within the classroom.
While the debate on sex and gender evolves at pace, children should not be caught in the crossfire. This report marks a new contribution to a growing body of evidence calling for the fundamental principles of child safeguarding to be re-prioritised within schools.
Next chapter2. Safeguarding principles
Safeguarding refers to the measures taken to ensure people – especially children and young people – are not put at undue risk of harm. As a concept, safeguarding is designed to encompass a holistic range of measures, including a minimum standard that must be met in order to ensure children are able to grow up in healthy and safe circumstances. Safeguarding is the responsibility of everyone who comes into contact with a child and their family. Safeguarding principles are well-established and considered to be vital in underpinning the operation of a safe and functioning society in the UK. As in all circumstances, safeguarding principles are a crucial lens through which to view gender-distressed children and the care they receive.
Safeguarding is defined by the government as:
- protecting children from maltreatment;
- preventing the impairment of children’s mental and physical health or development;
- ensuring that children grow up in circumstances consistent with the provision of safe and effective care; and
- taking action to enable all children to have the best outcomes.13WTTSC, pg.6.
The Children Acts of 1989 and 2004 provide the legislative framework for the requirements and expectations of child safeguarding in England. Section 11 of the Children Act 2004 states that any organisation or function providing services to children is legally required to promote their welfare and safeguard them:
‘Each person and body to whom this section applies must make arrangements for ensuring that—
(a)their functions are discharged having regard to the need to safeguard and promote the welfare of children; and
(b)any services provided by another person pursuant to arrangements made by the person or body in the discharge of their functions are provided having regard to that need.’14Children Act 2004, Part 2, General, Section 11. https://www.legislation.gov.uk/ukpga/2004/31/section/11
The government also provides several statutory documents which set out safeguarding duties on schools and public sector bodies. Working Together to Safeguard Children (2018) (WTTSC) outlines how all practitioners working with children (including teachers) should operate with regard to safeguarding.15Ibid. Practitioners refers to individuals who work with children in any capacity, including teachers. Keeping Children Safe in Education (2022) (KCSIE) outlines the safeguarding responsibilities schools and colleges have towards children within education settings.16Department for Education, Keeping Children Safe in Education 2022, 1 September 2022, pg.3. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/110145 4/Keeping_children_safe_in_education_2022.pdf
The Office for Standards in Education, Children’s Services and Skills (Ofsted) is a non-ministerial department within the government responsible for inspecting services that provide education and services for children and young people. In its 2017-2022 strategy, Ofsted highlighted that ‘Even more important than ensuring young people are learning well is ensuring they are kept safe.’17Ofsted, Ofsted strategy 2017-22, September 2017, pg.10. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/648212/Ofsted_strategy_2017-22.pdf Ofsted inspectors are required to assess every school’s safeguarding policies to ensure they are in line with the law and statutory guidance.18Ofsted, Education inspection framework, 11 July 2022. https://www.gov.uk/government/publications/education-inspection-framework/education-inspection-framework Ofsted expects every school to have ‘a culture of safeguarding.’19Ofsted, School inspection framework, 11 July 2022. https://www.gov.uk/government/publications/school-inspection-handbook-eif/school-inspection-handbook#safeguarding Every inspection involves a safeguarding assessment and contains a written judgement about the effectiveness of its safeguarding measures.20Ibid. A school will be automatically deemed to be inadequate if these measures are found to be ineffective.21Ofsted, School inspection handbook, September 2018. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/730127/School_inspection_handbook_section_5_270718.pdf
This chapter summarises safeguarding practice in six core elements: the emphasis on a whole school approach, the importance of multi-agency working, the adoption of a ‘it could happen here’ mentality, the practice of information sharing and parental involvement, as well as outlining groups of children the government understands to be particular safeguarding risks. All of these elements are important when discussing the provision of care for gender-distressed children in school.
2.1 A whole school approach
The responsibility for safeguarding rests with the senior leadership of a school, falling under governing bodies or proprietors – those that have strategic leadership responsibility. KCSIE states that all schools should take ‘a whole school approach’ to safeguarding:
‘This means involving everyone in the school or college, and ensuring that safeguarding, and child protection are at the forefront and underpin all relevant aspects of process and policy development. ’22KCSIE, pg.10.
As part of this approach, every school must have an annually reviewed, publicly available safeguarding policy that is transparent to staff, parents, carers and children, so that everyone in contact with children – including children themselves – can confidently raise any concerns. KCSIE recognises that a child will not necessarily always understand or have the ability to express if they are at risk of or are being harmed.23Ibid, pg.8. While taking into consideration a child’s wishes, a whole school approach always operates with ‘the best interests of the child at their heart.’24Ibid, pg.26. Implicit within this is the understanding that what is in the best interests of the child may not always be understood by the child themselves.
KCSIE requires every school to maintain a single central record (SCR), which records all pre-appointment staff checks. The minimum information that must be recorded includes identity checks, enhanced Disclosure and Barring Service (DBS) checks and checks regarding professional qualifications. The SCR covers all staff, including agency and third-party staff ‘even if they work for one day.’25Ibid, pg.70.
As part of the senior leadership team, every school should have a designated safeguarding lead (DSL). This post should oversee all safeguarding issues within a school, ensure all staff are trained in safeguarding protocol, as well as operate as the point of contact for external partners, with whom they should have established relationships. Without exception, the DSL should always be available to deal with safeguarding issues.26Ibid, pg.16.
Safeguarding principles work from the premise that children are inherently vulnerable, not the other way around. Safeguarding principles do not exist simply to respond to harm when it occurs but also to prevent harm to begin with. The way a child feels about a situation affecting them does not mitigate any safeguarding risk. This is particularly important with regard gender-distressed children, who may feel certain that social transition will solve their distress. This principle is clearly outlined in KCSEI:
‘All staff should be aware that children may not feel ready or know how to tell someone that they are being abused, exploited, or neglected, and/or they may not recognise their experiences as harmful.’27Ibid, pg. 8.
Safeguarding principles do not accept at face value that a child’s emotional understanding about a situation (regardless of what it is) offsets the risk of harm. All staff within school are required to respect this by conducting professional curiosity. Professional curiosity refers to the practice of exploring and understanding what is going on in a child’s life rather than accepting what a child says at face value. KCSIE refers to the importance of professional curiosity within safeguarding.28Ibid.
2.2 Multi-agency working
Schools are required to engage in multi-agency working, which involves co-operating fully with appropriate local authority partners in the local community to ensure no child is able to ‘slip through the net’ when it comes to child protection. Under Section 10 of the Children Act 2004, a local authority is expected to promote co-operation between itself and all functions working with children, including schools.29Children Act 2004, Part 2, General, Section 10. https://www.legislation.gov.uk/ukpga/2004/31/section/10 Similarly, schools are expected to have published protocol which sets out how they will work with other agencies; WTTSC outlines the statutory guidance which applies to any organisation or agency that relates to children. The document states: ‘We want a system that responds to the needs and interests of children and families and not the other way around. In such a system, practitioners will be clear about what is required of them individually, and how they need to work together in partnership with others.’30WTTSC, pg.6. Schools are expected to have clear systems in place that all staff recognise and understand, so that every concern can be appropriately escalated to relevant partners where necessary. KCSIE emphasises the role of schools and colleges in working with the local authority, children’s social care, the police, health services and others to promote the welfare of children. Point 113 states: ‘This includes providing a coordinated offer of early help when additional needs of children are identified and contributing to inter-agency plans to provide additional support to children subject to child protection plans.’31KCSIE, pg.30.
Safeguarding principles recognise that individual teachers will not always be best placed to resolve a safeguarding concern when it is raised. The emphasis on multi-agency working therefore protects both teachers and children. It protects teachers from being ill-equipped to deal with a particular issue, and ensures children receive appropriate service provision as soon as possible. The principle of multi-agency working is particularly important with regard to gender-distressed children at school. This will be explained in more depth in chapter eight. However, given the nature of gender-distress is inherently medical, it is important that schools recognise their role as part of a wider network of services in providing for a gender-distressed child.
2.3 ‘It could happen here’ mentality
Embedded within the concept of safeguarding is the premise that every adult has the potential to harm a child. This means that no one practitioner should be entirely responsible for safeguarding lest that duty be abused or neglected. KCSIE notes that ‘Staff working with children are advised to maintain an attitude of ‘it could happen here’ where safeguarding is concerned.’32Ibid, pg.16. Safeguarding principles do not accept that because someone might appear to be harmless, they should be considered so. School safeguarding organisation Safe Schools Alliance highlights this: ‘you never know anyone well enough to say they couldn’t, wouldn’t or didn’t’.33Safe Schools Alliance UK, The Sheldon Report: has anything changed? 18th March 2021. https://safeschoolsallianceuk.net/2021/03/18/the-sheldon-report/ Rather, safeguarding works from the premise that every person must be regularly assessed and assumed to have the capacity to cause harm, regardless of their current or past experience with children.
2.4 Information sharing
Underpinning multi-agency working is the sharing of information, which is a foundational principle of child safeguarding. Schools are afforded clear powers to share and use information for the purpose of keeping children safe. Paragraph 16 of WTTSC states:
‘Everyone who works with children has a responsibility for keeping them safe. No single practitioner can have a full picture of a child’s needs and circumstances and, if children and families are to receive the right help at the right time, everyone who comes into contact with them has a role to play in identifying concerns, sharing information and taking prompt action.’34WTTSC, pg.11.
Information sharing should be the default position over confidentiality when it comes to child protection, and all statutory guidance is clear that data protection laws do not prohibit the sharing of information with regard to child protection. Schedule 1 of The Data Protection Act 2018 itself states ‘safeguarding of children and individuals at risk’ as a processing condition, which enables practitioners to share information without consent.35Data Protection Act 2018, Schedule 1. https://www.legislation.gov.uk/ukpga/2018/12/schedule/1/enacted Related to this, is the principle that confidentiality should never be promised to children themselves. KCSIE states this specifically: ‘Staff should never promise a child that they will not tell anyone about a report of any form of abuse, as this may ultimately not be in the best interests of the child.’36KCSIE, pg.8.
In 2018, the government published Information sharing: Advice for practitioners providing safeguarding services to children, young people, parents and carers, which outlines six principles intended to help practitioners working with children and their families to appropriately share information.37HM Government, Information sharing: Advice for practitioners providing safeguarding services to children, young people, parents and carers, July 2018, pg.9.https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1062969/Information_sharing_advice_practitioners_safeguarding_services.pdf
The government’s information sharing principles for child practitioners
- Relevant – only relevant information to the safeguarding concern should be shared.
- Adequate – information needs to be ‘adequate for its purpose’ and understandable.
- Accurate – information should be accurate and ‘clearly distinguish between fact and opinion’.
- Timely – information must be shared promptly and appropriately once a safeguarding concern has been recognised.
- Secure – information should be shared securely.
- Record – all information should be recorded. There should never be a situation where a safeguarding concern is not recorded.38Ibid.
For the purposes of this report, all six principles are essential when a child discloses feelings of gender distress to a teacher. However, particularly important are the principles of timeliness and record-keeping. As soon as a child discloses feelings of gender distress, standard safeguarding practice would expect a teacher to share this information with relevant individuals immediately. The conversation would also not be considered confidential or colloquial. Rather, it would be documented and stored on the school’s Information Management System (IMS).
2.5 Parental responsibility
The Children Act of 1989 states explicitly that parental involvement in the life of their child is paramount. No other body is to assume parental responsibility for a child unless the court intervenes. While by default, parents are accepted to be the most emotionally and financially invested in their child’s welfare, safeguarding principles do recognise that there are exceptions to this, such as where a child is being actively harmed – or at risk of harm – because of their parents.39The Children Act 1989 introduced the concept of Significant Harm – the threshold that justifies compulsory intervention in the family life of a child where it is in the best interests of the child. Children Act 1989, Part IV, General, Section 31. https://www.legislation.gov.uk/ukpga/1989/41/section/31
The law is clear that parental involvement in a child’s life should be prioritised. Parental responsibility “means all the rights, duties, powers, responsibilities and authority which by law a parent of a child has in relation to the child and his property’.40Ibid, Part I, Section 3. https://www.legislation.gov.uk/ukpga/1989/41/section/3 Those who have parental responsibility for a child should be empowered to make decisions for that child and receive information about them. This is especially important for the sake of children who disclose gender-distress at school.
The Government defines parental responsibility as:
- providing a home for the child
- protecting and maintaining the child
- disciplining the child
- choosing and providing for the child’s education
- agreeing to the child’s medical treatment
- naming the child and agreeing to any name change
- looking after child’s property
- supporting the child financially.41Gov.UK, Parental rights and responsibilities. https://www.gov.uk/parental-rights-responsibilities
The government’s emphasis on parental responsibility regarding a child’s education, health, and agreeing to a name change is particularly relevant to this report, as all three of these responsibilities are affected by the affirmative approach to gender distress. WTTSC states that a child-centered approach to safeguarding must respect the principles of the Children Acts 1989 and 2004, confirming that children are best placed with their families ‘with their parents playing a full part in their lives, unless compulsory intervention in family life is necessary.’42WTTSC, pg.9. KCSIE references the importance of informing parents where safeguarding issues are raised, unless there are reasonable grounds not to (again, if the safeguarding concern related directly to the child’s parents themselves).
There is a further legal duty on local authorities based on The Education Act of 1996 relating to parental involvement in a child’s education. Chapter 1, section 9 states that ‘local authorities shall have regard to the general principle that pupils are to be educated in accordance with the wishes of their parents’.43Education Act 1996, Part I, Chapter I, Education in accordance with parental wishes. https://www.legislation.gov.uk/ukpga/1996/56/part/I/chapter/I/crossheading/education-in-accordance-with-parental-wishes Open communication between parents and their child’s school is therefore paramount. If a child discloses information that is not known by their parents, their school is required to disclose this information and to act in accordance with the wishes of the parent – unless there is a safeguarding risk.
As with every other mental health issue, parents should be informed if a child discloses gender-distress at school, even if a child would rather their parents did not know. Given the fact that many schools are failing to recognise the medical nature of gender distress and affirmative practice, many schools are not automatically informing parents when this issue arises. This will be explained in greater depth later, but a parent who does not feel affirmation at school is the right course of treatment for their child does not constitute risk. Schools should work with the parents of a gender-distressed child as they would do in every other safeguarding circumstance.
2.6 Particular safeguarding risks
KCSIE outlines a number of particular characteristics and situations that could present a safeguarding risk for a child. These include the need for early safeguarding intervention for a child who:
- ‘is disabled or has certain health conditions and has specific additional needs
- has special educational needs (whether or not they have a statutory Education, Health and Care Plan)
- has a mental health need
- is a young carer
- is showing signs of being drawn in to anti-social or criminal behaviour, including gang involvement and association with organised crime groups or county lines
- is frequently missing/goes missing from care or from home
- is at risk of modern slavery, trafficking, sexual or criminal exploitation
- is at risk of being radicalised or exploited
- has a family member in prison, or is affected by parental offending
- is in a family circumstance presenting challenges for the child, such as drug and alcohol misuse, adult mental health issues and domestic abuse
- is misusing alcohol and other drugs themselves
- has returned home to their family from care
- is at risk of ‘honour’-based abuse such as Female Genital Mutilation or Forced Marriage
- is a privately fostered child, or
- is persistently absent from education, including persistent absences for part of the school day.’44KCSIE, pg.9. Emphasis added.
The circumstances above that are emphasised are overrepresented in the current caseload of children presenting with gender distress. Consequently, many children reporting that they experience gender distress should already be considered to be an additional safeguarding risk.
The document also notes that staff should be aware that these situations or characteristics and safeguarding issues ‘are rarely standalone events and cannot be covered by one definition or one label alone. In most cases, multiple issues will overlap with one another.’45Ibid, pg.15.
2.6.1 Dealing with mental health issues
There is a strong link between poor mental health and gender-distress, which will be expanded on later. KCSIE outlines specifically how teachers should deal with a child’s mental health problem.
Paragraph 46 of the document again promotes the need for multi-agency working, specifying that:
‘Only appropriately trained professionals should attempt to make a diagnosis of a mental health problem…Schools and colleges can access a range of advice to help them identify children in need of extra mental health support, this includes working with external agencies.’46Ibid.
On identifying a mental health concern, teachers must take immediate action, ‘following their child protection policy, and speaking to the designated safeguarding lead or a deputy.’47Ibid.
Next chapter3. Relationships and Sex Education and Health Education (RSHE)
Related to how well schools are upholding safeguarding standards for gender-distressed children is what they are teaching about sex and gender. This section will summarise key elements of the government’s guidance on Relationships and Sex Education (RSHE) and Health Education.
The government released the statutory guidance Relationships Education, Relationships and Sex Education (RSE) and Health Education in 2019. The following year, Relationships Education, Relationships and Health Education was made compulsory in all primary and secondary schools.48Department for Education, Relationships Education, Relationships and Sex Education (RSE) and Health Education, Statutory guidance for governing bodies, proprietors, head teachers, principals, senior leadership teams, teachers, last updated 13 September 2021. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1090195/Relationships_Education_RSE_and_Health_Education.pdf
While schools are able to determine their own curriculum, they must have regard to the guidance, ‘and where they depart from those parts of the guidance which state that they should (or should not) do something they will need to have good reasons for doing so.’49Ibid, pg.6. As with all subject matter, the guidance is clear that ‘at the heart of these subjects there is a focus on keeping children safe’.50Ibid, pg.42. By the end of secondary school, the guidance states that pupils should know: ‘the legal rights and responsibilities regarding equality (particularly with reference to the protected characteristics as defined in the Equality Act 2010) and that everyone is unique and equal.’51Ibid, pg.28. This includes understanding the difference between the protected characteristics of ‘sex’ and ‘gender reassignment’.
Schools also have a legal obligation to be politically impartial. Sections 406 and 407 of the Education Act 1996 state that schools are prohibited from promoting partisan political views, and that where political viewpoints are raised, children ‘are offered a balanced presentation of opposing views.’52Education Act 1996, Part Five, Chapter IV, Politics, Section 407. https://www.legislation.gov.uk/ukpga/1996/56/section/407 Further government information aimed at helping schools plan and implement the RSHE curriculum state that schools must comply with the Human Rights Act 1998, which protects the right to freedom of expression.53Gov.UK, Plan your relationships, sex and health curriculum, 24 September 2020. https://www.gov.uk/guidance/plan-your-relationships-sex-and-health-curriculum#using-external-agencies In February 2022, following public concerns that schools were not being sufficiently political impartial, the government released guidance on how schools should explicitly navigate teaching with regard to political issues and movements.54Gov.UK, Political impartiality in schools, 17 February 2022. https://www.gov.uk/government/publications/political-impartiality-in-schools/political-impartiality-in-schools#using-external-agencies
On specific curriculum content regarding sex and gender, further DfE non-statutory guidance states:
‘You should not reinforce harmful stereotypes, for instance by suggesting that children might be a different gender based on their personality and interests or the clothes they prefer to wear. Resources used in teaching about this topic must always be age-appropriate and evidence based. Materials which suggest that non-conformity to gender stereotypes should be seen as synonymous with having a different gender identity should not be used and you should not work with external agencies or organisations that produce such material. While teachers should not suggest to a child that their non-compliance with gender stereotypes means that either their personality or their body is wrong and in need of changing, teachers should always seek to treat individual students with sympathy and support.’55Gov.UK, Plan your relationships, sex and health curriculum, 24 September 2020.
RSHE guidance re-iterates the importance of parental involvement in a child’s life at school. With regard to RSHE, statutory guidance states:
‘The role of parents in the development of their children’s understanding about relationships is vital. Parents are the first teachers of their children. They have the most significant influence in enabling their children to grow and mature and to form healthy relationships.’56Department for Education, Relationships Education, Relationships and Sex Education (RSE) and Health Education, Statutory guidance for governing bodies, proprietors, head teachers, principals, senior leadership teams, teachers, last updated 13 September 2021, pg.17. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1090195/Relationships_Education_RSE_and_Health_Education.pdf
Schools are obliged to work closely with parents such that they have confidence in the curriculum and understand the importance of RSHE: ‘It is important through such processes to reach out to all parents, recognising that a range of approaches may be needed for doing so.’57Ibid.
Regarding teaching materials, guidance states: ‘Schools should also ensure that, when they consult with parents, they provide examples of the resources that they plan to use as this can be reassuring for parents and enables them to continue the conversations started in class at home.’58Relationships Education, Relationships and Sex Education (RSE) and Health Education, pg.13.
There are sensitive reasons why a parent may feel uncomfortable with their child receiving elements of RSHE, particularly regarding sex education. Both parents’ and students’ right to freedom of expression under the European Convention on Human Rights (ECHR) should be protected, as well as tolerance and understanding that some ideas taught within RSHE may conflict with a pupil’s or their parents’ religious or gender critical beliefs. In a recent judgement handed by the Employment Appeals Tribunal (EAT), gender critical belief is protected under Section 10 of the Equality Act 2010.59Forstater v CGD Europe, Center for Global Development and Masood Ahmed, Employment Tribunal, Case No. 22000909/2019, 2022. https://www.judiciary.uk/judgments/maya-forstater-v-cgd-europe-center-for-global-development-masood-ahmed/ Section 10 is concerned with the protected characteristic of religion or belief.60Equality Act 2010, Part 2, Chapter 1, Section 10. https://www.legislation.gov.uk/ukpga/2010/15/section/10
Furthermore, the ‘right to respect for private and family life’ is expressed through Article 8 of the Human Rights Act, given effect to the human rights set out in the ECHR.61Equality and Human Rights Commssion, Article 8: Respect for your private and family life, last updated 24 June 2021. https://www.equalityhumanrights.com/en/human-rights-act/article-8-respect-your-private-and-family-life This means that everyone has the right to live their life privately without government interference, and that every family has the right to maintain family relationships, including between parents and their children.62Ibid.
The right to withdraw should be respected: parents can request that their child is withdrawn from as little or as much of the sex education element of RSHE as they wish.63Relationships Education, Relationships and Sex Education (RSE) and Health Education, pg.17. Parents do not have a right to withdraw their child from Relationships or Health Education. Prior to withdrawal, guidance advises the school’s headteacher to discuss this decision with parents and students.64Ibid.
3.1 Using external agencies
External agencies are permitted to deliver RSHE, however there are obligations on schools to ensure external providers are both politically impartial and aligned with the school’s wider safeguarding standards. The government guidance Plan your relationships, sex and health curriculum outlines extensively how external agencies should be engaged with, in order to ensure RSHE is taught appropriately. Schools are obliged to ‘exercise extreme caution when working with external agencies’.65Gov.UK, Plan your relationships, sex and health curriculum. It also states that: ‘schools should not under any circumstances work with external agencies that take or promote extreme political positions or use materials produced by such agencies.’66Ibid. This point is especially important for the purposes of this report, because many of the external resources and agencies schools are using regarding teaching on sex and gender have explicitly political aims, such as embedding gender identity beliefs in the law.
Schools using external agencies to deliver RSHE are obliged to ensure:
|
4. The gender-affirmative approach
Having summarised the UK’s safeguarding standards and guidance on teaching RSHE, this section will look at the affirmative approach towards children with gender distress. The WHO defines gender affirming care as ‘any single or combination of a number of social, psychological, behavioural or medical (including hormonal treatment or surgery) interventions designed to support and affirm an individual’s gender identity.’110World Health Organisation, Gender incongruence and transgender health in the ICD. https://www.who.int/standards/classifications/frequently-asked-questions/gender-incongruence-and-transgender-health-in-the-icd Within healthcare, the gender affirmative care pathway can involve several forms of medical intervention, and is available both on the NHS and privately. Gender affirmative care is common for both children and adults in the UK. This was highlighted by the Interim Cass Report, which concluded that the current and soon to be defunct GIDS has primarily adopted a gender affirmative approach. It states:
“From the point of entry to GIDS there appears to be predominantly an affirmative, non-exploratory approach, often driven by child and parent expectations and the extent of social transition that has developed due to the delay in service provision.”111The Cass Review, pg.17.
Social transition is often considered a ‘first line’ form of medical intervention in which a child transitions to live with attributes associated with the opposite sex. For example, this could entail adopting a new name, pronouns, different clothing or hairstyle. Teenage girls may also flatten their breasts through wearing a ‘binder’ or exhibiting a ‘packer’ to give the appearance of having male genitalia. The long-term side effects of chest binding in girls whose breasts have not yet matured is unknown, but in a study of nearly 2000 participants, over 97 per cent experienced some kind of negative side effect, including chest pain, shortness of breath, and scarring.112S. Peitzmeier, I. Gardner, J. Weinand et al, Health impact of chest binding among transgender adults: a community-engaged, cross-sectional study, Cult Health Sex. 2017 Jan;19(1):64-75. https://pubmed.ncbi.nlm.nih.gov/27300085/ Many children choose to socially transition in certain settings, such as only at home or school, or social transition may be exhibited full-time. A likely consequence of social transition and a further element of gender affirmative care is hormonal and surgical treatment to change a person’s body to more closely resemble the opposite sex. GIDS offers a model of care which consists of four stages. The first stage is an assessment which aims ‘to gather a holistic view of the child or young person’s life’ which includes exploring their history of gender distress, family history and other factors.113Gender Identity Development Service, Thinking about the body. https://gids.nhs.uk/young-people/puberty-and-physical-intervention/ At the end of this assessment, referral to an endocrinologist (hormone specialist) may be made, if it is felt that continuing with transition will resolve dysphoria.
The prescription of puberty blockers is a further intervention advocated for by affirmative practice. Puberty blockers are prescribed to halt pubertal changes associated with biological sex. According to stage two of GIDS pathway, blockers are prescribed to allow children time to consider more fully their gender identity and reduce gender distress by halting the development of the secondary sex characteristics that come with puberty.114Ibid. Puberty blockers can be prescribed in children who reach
Tanner stage two, which can begin in a child as early as age eight. GIDS claims that blockers are ‘physically reversable interventions’ because once a child ceases to take them, their body should continue to develop as it would have done.115Ibid. This claim is unsubstantiated, as outlined in the Interim Cass Report, which highlighted the fact that social transition ‘may have significant effects on the child or young person in terms of their psychological functioning.’116The Cass Review, pg.62.
The idea behind such early medical intervention is based on the ‘Dutch protocol’ (DP) conducted in 1998. The protocol was based on the thesis that gender-distressed children may have better outcomes if they began treatment before they became adults. The results of the study appeared positive.117M. Biggs, The Dutch Protocol for Juvenile Transsexuals: Origins and Evidence, Journal of Sex & Marital Therapy, 19 September 2022, pg.1. https://www.tandfonline.com/doi/pdf/10.1080/0092623X.2022.2121238 Subsequently, the prescription of puberty blockers for younger children became the international standard for treating gender dysphoria. In recent years the protocol has been discredited, on the basis that the study had serious methodological flaws, principally the fact that it only included positive outcomes in its results.118Ibid, pg.9. It also judged success on how well puberty blockers supressed puberty in gender-dysphoric teenagers, not how well they resolved their gender dysphoria. On the basis that puberty blockers had halted their genitals from developing enough for standard cross-sex surgery to take place safely, one participant died as a result of pubertal suppression. This patient’s case was omitted from the final study.119Ibid, pg.8.
The NHS approach is based on the Dutch model, however there are substantial differences between the two, as noted by the Cass Interim Report. Notably, that within the Dutch model, routine therapeutic support is given to gender-distressed neurodiverse children or those with mental health conditions. This is not the case within the NHS. As Cass notes: ‘criteria to have accessed therapeutic support prior to starting hormone blocking treatment do not appear to be integral to the current NHS process.’120The Cass Review, pg.18.
Despite claiming that blockers are reversible, GIDS acknowledges that the physical and psychological long-term effects of blockers in this clinical context are unknown.121Gender Identity Development Service, Thinking about the body This is demonstrated in an evidence review conducted by the National Institute for Health and Care Excellence (NICE) in 2021.122The Cass Review, Nice Evidence Reviews. https://cass.independent-review.uk/nice-evidence-reviews/ Several academic studies suggest that the effects of puberty blockers are in fact irreversible and significantly affect the development of the adolescent brain.123M. Biggs, The Dutch Protocol for Juvenile Transsexuals: Origins and Evidence, pg.3.
In 2020, former GIDS patient Kiera Bell lodged a complaint against the service, on the basis that they prescribed her puberty blockers aged 16 without gaining her informed consent. Prior to her case, a child could be prescribed puberty blockers without parental consent. While the High Court initially ruled that children under 16 were unlikely to be able to give informed consent to receive puberty blockers, on appeal the ruling was quashed.124Bell v Tavistock and Portman NHS Foundation Trust [2020] EWHC 3274 (Admin). https://www.judiciary.uk/wp-content/uploads/2022/07/Bell-v-Tavistock-judgment-170921.pdf However, GIDS policy is now that every under-16’s case must go through an internal ‘Multi-Professional Review Group’. The purpose of this is ‘not to endorse or refuse treatment but to ensure the necessary steps have been taken and information has been provided to the patient and their parents/carers.’125Gender Identity Development Service, Thinking about the body In the UK, puberty blockers are not licensed to treat gender dysphoria. They are licensed to treat prostate cancer, precocious puberty and endometriosis.126National Institute for Health and Care Excellence, Gonadotophins. https://bnf.nice.org.uk/treatment-summaries/gonadotrophins/
Another medical intervention supported by a gender affirmative approach is the prescription of irreversible cross-sex hormones (testosterone or oestrogen), with the aim of producing some of the secondary sex characteristics developed by the opposite sex. While GIDS refers to cross-sex hormones as stage three of the medical pathway they offer, most children who take puberty blockers will go onto take cross-sex hormones, and so the distinction between the stages is minimal. In a GIDS study from 2021, of 44 children who received puberty blockers, 43 went onto take cross-sex hormones (98 per cent).127P.Carmichael, G. Butler, U. Masic et al, Short-term outcomes of pubertal suppression in a selected cohort of 12 to 15 year old young people with persistent gender dysphoria in the UK, PLoS ONE 16(2): e0243894, February 2021. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0243894 An FOI response from Leeds General Infirmary found that in 2019, 78 of 87 (90 per cent) of children took the same route.128WhatDoTheyKnow, Prescribing hormones and puberty blockers to transgender children, 17 February 2020. https://www.whatdotheyknow.com/request/prescribing_hormones_and_puberty
These findings led the Cass Interim Report to question whether puberty blockers are actually just a ‘pause button’ or “whether they effectively ‘lock in’ children and young people to a treatment pathway which culminates in progression to feminising/masculinising hormones by impeding the usual process of sexual orientation and gender identity development.”129The Cass Review, pg.38. The long-term effects of cross-sex hormones are considerable. Temporary (or sometimes permanent) infertility, higher risk of cancer and blood clots are commonly reported.130NHS, Treatment: Gender dysphoria, last updated 28 May 2020. https://www.nhs.uk/conditions/gender-dysphoria/treatment/ A recent study suggests that those who take cross-sex hormones are nearly seven times more likely to suffer a stroke, and nearly six times more likely to suffer from a severe heart attack.131American College of Cardiology, Hormone Therapy for Gender Dysphoria May Raise Cardiovascular Risks, 23 February 2023. https://www.acc.org/About-ACC/Press-Releases/2023/02/22/20/29/Hormone-Therapy-for-Gender-Dysphoria-May-Raise-Cardiovascular-Risks GIDS will prescribe cross-sex hormones at age 16 once a child has been taking puberty blockers for a year. If blockers are found to prevent psychological maturing of the brain, it follows that a child may not be in a competent state of maturity to make the decision to carry onto cross-sex hormones, despite the fact that taking blockers is the necessary criteria to be prescribed them. As with puberty blockers, they are not licensed for the treatment of gender dysphoria in the UK.132National Institute for Health and Care Excellence, Sex hormones. https://bnf.nice.org.uk/treatment-summaries/sex-hormones/
The final medical intervention approved by an affirmative clinical pathway is surgical procedure, often referred to as sex reassignment surgery. According to the NHS, this pathway can be recommended to people once they have lived in their ‘preferred gender’ for at least a year.133NHS, Treatment: Gender dysphoria. Surgeries for transgender men (biological women) involve mastectomy, phalloplasty and hysterectomy. Surgery for transgender women (biological men) includes orchidectomy, penectomy and vaginoplasty. All of these procedures are available on the NHS once a person reaches 18.134NHS, Treatment: Gender dysphoria. GIDS does not offer any surgical procedures, however it is possible for under 18s to access surgery abroad.135One example is Boston Children’s Hospital, which ‘provides a full suite of surgical options for transgender teens and young adults’. This excludes genital surgery. They offer an international service. Boston Children’s Hospital, Center for Gender Surgery. https://www.childrenshospital.org/programs/center-gender-surgery-program There are serious risks involved with sex-reassignment surgery. In a study of 100 participants, it was found that long-term, one in ten died and one in three experienced somatic morbidity.136R. Simonsesn, G. Hald, E.Kristensen et al, Long-Term Follow-Up of Individuals Undergoing Sex-Reassignment Surgery: Somatic Morbidity and Cause of Death, Sexual Medicine, Volume 4, Issue 1, March 2016. https://www.sciencedirect.com/science/article/pii/S205011611600009X Other than social transition, the medical interventions involved with gender-affirmative care are lifelong because to maintain their effect, a person has to take cross-sex hormones and puberty blockers for life.137NHS, Treatment: Gender Dysphoria. https://www.nhs.uk/conditions/gender-dysphoria/treatment/
| Private provision
There are a growing number of private gender clinics in the UK. GenderGP is a private clinic based in Singapore which offers gender services to children online. Patients can pay a one-off fee of £195 which covers unlimited medical advice and private prescriptions.138GenderGP, Welcome to GenderGP. https://www.gendergp.com/wp-content/uploads/2021/08/Masculinising.pdf This fee enables a patient to begin their medical transition. There is no obligatory counselling or assessment required of patients in order to begin their medical transition, aside from a one-off Information Gathering Session which takes place online. Counsellors that conduct these sessions are not medically qualified.139GenderGP, Yes, You Are Trans Enough! 26 August 2020. https://www.gendergp.com/gendergps-approach-to-assessments-yes-you-are-trans-enough/ The founders of the clinic Dr Helen Webberly and Dr Michael Webberly were found guilty of medical negligence in a tribunal in May 2022 for providing inadequate care to gender-distressed children. In June 2022, Dr Helen Webberly was suspended from practicing for two months, while Dr Michael Webberly was struck off the medical register.140C.Dyer, Retired consultant is struck off over treatment of young transgender patients, BMJ, 30 May 2022. https://www.bmj.com/content/377/bmj.o1357 The clinic remains in operation. Sex-reassignment surgery and its add-ons have become a lucrative market, and is expected to be worth $1.9bn globally by 2032.141Global Market Insights, Sex Reassignment Surgery Market, January 2023. https://www.gminsights.com/industry-analysis/sex-reassignment-surgery-market There are various surgical procedures available privately, including face feminisation, laser hair removal and breast augmentation. |
As aforementioned, in February 2022 Dr Cass’ independent interim review into GIDS found the current model of care to be neither ‘safe or viable’.142The Cass Review, pg.20. The report found there to be a serious issue of diagnostic overshadowing:
‘many of the children and young people presenting have complex needs, but once they are identified as having gender-related distress, other important healthcare issues that would normally be managed by local services can sometimes be overlooked.’143Ibid, pg.17
Furthermore, Dr Cass found that ‘at primary, secondary and specialist level, there is a lack of agreement, and in many instances a lack of open discussion’ about the causes of gender distress, and therefore how to deal with it.144Ibid, pg.16 Despite the lack of agreement on the causes of gender distress, it appears that the service advocated primarily for only one solution: ‘From the point of entry to GIDS there appears to be predominantly an affirmative, non-exploratory approach.’145Ibid, pg.17. A lack of safeguarding protocol with regard to working with external agencies when concerns were raised was also highlighted by the report.146Ibid.
In a letter to NHS England, Dr Cass recommended regional centres should be established within specialist children’s hospitals. Dr Cass emphasised safeguarding as a key component of the new model:
‘There should also be expertise in safeguarding, support of looked-after children and children who have experienced trauma. Staff should maintain a broad clinical perspective by working across related services within the tertiary centre and between tertiary and secondary centres in order to embed the care of children and young people with gender-related distress within a broader child and adolescent health context.’147The Cass Review, Letter to NHS England – January 2023, 31 January 2023. https://cass.independent-review.uk/publications/
In July 2022, the NHS announced that it would be implementing the recommendations of the Interim Cass Report, and replacing the current service with a regional model of care.148NHS England, Implementing advice from the Cass Review. https://www.england.nhs.uk/commissioning/spec-services/npc-crg/gender-dysphoria-clinical-programme/implementing-advice-from-the-cass-review/ Several countries are moving away from the affirmative model of care, including Sweden,149Society for Evidence Based Gender Medicine, Sweden’s Karolinska Ends All Use of Puberty Blockers and Cross-Sex Hormones for Minors Outside of Clinical Studies, 5 May 2021. https://segm.org/Sweden_ends_use_of_Dutch_protocol Finland150Society for Evidence Based Gender Medicine, One Year Since Finland Broke with WPATH “Standards of Care”, 2 July 2021. https://segm.org/Finland_deviates_from_WPATH_prioritizing_psychotherapy_no_surgery_for_minors and France.151Society for Evidence Based Gender Medicine, National Academy of Medicine in France Advises Caution in Pediatric Gender Transition, 3 March 2022. https://segm.org/France-cautions-regarding-puberty-blockers-and-cross-sex-hormones-for-youth
Next chapter5. The ‘watchful waiting’ approach
Contrary to the affirmative model towards gender-distressed children common within UK clinical settings and schools, is an approach termed ‘watchful waiting’. Watchful waiting describes an approach to a medical problem in which time passes before medical intervention is prescribed. It is applied for both mental and physical health conditions.
In the context of gender distressed children, watchful waiting is a therapeutic approach that does not affirm a child’s belief that they are the opposite gender through any kind of active intervention such as social transition. Sometimes, children will be helped to feel more comfortable with their sexed body, but the position starts from the premise that developmental change is an inevitable part of growing up. Psychologist and expert in gender dysphoria Dr Kenneth Zucker is often seen as the foundational psychologist behind the watchful waiting approach.176A. Shrier, Irreversible Damage: The Transgender Craze Seducing Our Daughters, Regenery Publishing (2020), pg.123. Having worked with hundreds of children experiencing gender-distress, Dr Zucker recognised that rates of mental distress in gender-distressed children are comparable to those in children with other psychiatric disorders of ‘an internalised nature’, such as depression and anxiety.177S. Bradley, K. Zucker, Gender Identity Disorder: A Review of the Past 10 Years, Journal of the American Academy of Child & Adolescent Psychiatry, Volume 36, Issue 7, July 1997. https://www.jaacap.org/article/S0890-8567(09)62542-9/pdf Subsequently, a child’s gender-distress is most often a symptom of something else going on, not necessarily a cause in and of itself.178Ibid. Watchful waiting therefore takes a holistic approach (similarly to other mental health disorders) in which a child may be given therapy that focuses on resolving co-existing problems in their life, rather than simply attempting to solve the single issue of the dysphoria through affirmation.179J.Ristori & T.Steensma, Gender dysphoria in childhood, International Review of Psychiatry 28:1, 13-20 (2016). https://doi.org/10.3109/09540261.2015.1115754, pg.17. As the next chapter will demonstrate, it is very common for gender distressed or dysphoric children to present with other contributing factors.
‘Desistence’ and ‘persistence’ are the terms given to children who do or do not outgrow gender distress with age. There is a growing body of evidence which suggests the majority of children desist and do not transition in adulthood.180T.Steensma, J.McGuire, B.Kreukels et al, Factors associated with desistence and persistence of childhood gender dysphoria: a quantitative follow-up study, J Am Acad Child Adolesc Psychiatry, 2013 Jun;52(6):582-90. https://pubmed.ncbi.nlm.nih.gov/23702447/ and T.Steensma, R.Biemond, F.de Boar et al, Desisting and persisting gender dysphoria after childhood: A qualitative follow-up study, Clinical Child Psychology and Psychiatry 16(4):499-516. https://www.researchgate.net/publication/49738851_Desisting_and_persisting_gender_dysphoria_after_childhood_A_qualitative_follow-up_study and M.Wallien & P.Cohen-Kettenis, Psychosexual Outcome of Gender-Dysphoric Children, Journal of the American Academy of Child & Adolescent Psychiatry, Volume 47, Issue 12, December 2008, Pages 1413-1423. https://www.sciencedirect.com/science/article/abs/pii/S0890856708601422 In the largest study of natal boys to date referenced above, 87 per cent had desisted when followed up 13 years later.181D.Singh, S.Bradley & K.Zucker, A Follow-Up Study of Boys With Gender Identity Disorder. Watchful waiting has been very successful in resolving gender distress. In an analysis of ten studies that focused on the persistence of gender dysphoria, over 85 per cent of children found their dysphoria was resolved without any form of medical intervention, including social transition.182J.Ristori & T.Steensma, Gender dysphoria in childhood, pg.15. Furthermore, nearly 30 per cent of transgender patients, in a study of 1000, were found to have desisted when followed up after four years. This means that nearly three in ten participants had taken irreversible medical intervention before desisting to their biological sex.183C. Roberts, D. Klein, T.Adirim et al, Continuation of Gender-affirming Hormones Among Transgender Adolescents and Adults, J Clin Endocrinol Metab, 2022 Aug 18;107(9):e3937-e3943. https://pubmed.ncbi.nlm.nih.gov/35452119/
Next chapter6. Gender Distress in Context
The Interim Cass Report notes that ‘children and young people presenting to gender identity services are not a homogeneous group’.184The Cass Review, pg.27.
There are a number of trends and subgroups in the clinical caseload of children needing provision for gender distress. There is a lack of data and research on these subgroups, and the recency of the phenomenon means long-term follow up data is not readily available. It is also worth noting that there will be significant numbers of children presenting with gender distress who are not referred to GIDS or diagnosed with gender dysphoria, which means gaining a full picture of the scale of the situation is difficult. The unprecedented numbers of children needing treatment has overwhelmed the current service. As of July 2022, there were nearly 8000 children waiting for an initial appointment.185NHS England, NHS England: Equality and Health Inequalities Impact Assessment (EHIA), 12 October 2022. https://www.engage.england.nhs.uk/specialised-commissioning/gender-dysphoria-services/user_uploads/b1937_iii_equalities-health-impact-assessment-interim-service-specification.pdf Natal females, looked after children, children with autism and children questioning their sexuality are overrepresented in the current caseload.
Referrals, 2011-12 to 2021-22
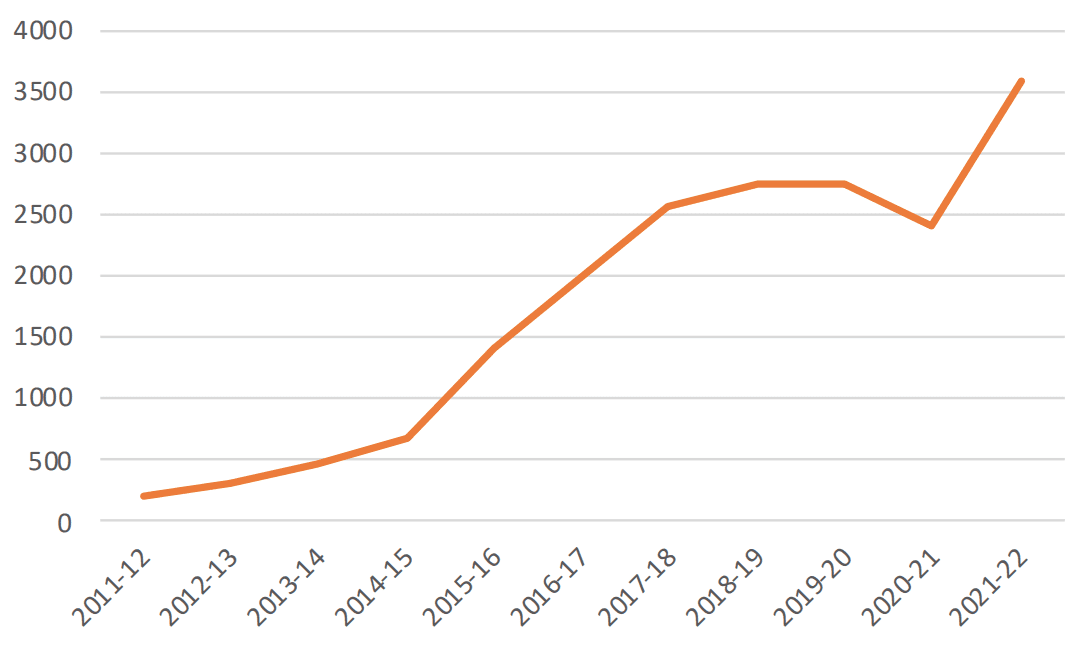
Source: GIDS data 186Gender Identity Development Service, Number of referrals to GIDS. https://gids.nhs.uk/about-us/number-of-referrals/
It is important to note that all of these groups (with the general exception of the first caseload trend – girls) have additional safeguarding needs, as outlined in a previous chapter. It is clear that gender distress is not reducible to one problem, and for children who fall within one or more of these subgroups, safeguarding practice should not be seen as isolated or irrelevant. Understanding the context of the current caseload should be central in assessing whether a treatment pathway appropriately conforms with safeguarding measures.
6.1 Overrepresentation of girls
Natal girls are hugely overrepresented in the number of referrals to GIDS. Publicly available GIDS data begins in 2010/11, when the number of natal male referrals was higher. Every year since, natal female referrals have consistently outweighed male referrals, and in 2016, numbers dramatically increased (by 118 per cent).187Ibid. This pattern is mirrored in caseloads in different countries such as in Finland, Sweden and New Zealand.188Finland: R.Kaltiala-Heino, M.Sumia, M.Työläjärvi et al, Two years of gender identity service for minors: overrepresentation of natal girls with severe problems in adolescent development, Child Adolescent Psychiatry and Mental Health, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4396787/. Sweden: Society for Evidence Based Gender Medicine, Summary of Key Recommendations from the Swedish National Board of Health and Welfare (Socialstyrelsen/NBHW), 27 February 2022 https://segm.org/segm-summary-sweden-prioritizes-therapy-curbs-hormones-for-gender-dysphoric-youth. New Zealand: J. Delahunt, H. Denison, D. Sim et al, Increasing rates of people identifying as transgender presenting to Endocrine Services in the Wellington region, N Z Med J. 2018 Jan 19;131(1468):33-42 https://pubmed.ncbi.nlm.nih.gov/29346355/. In terms of age-range, before age 12, the number of referrals remains below 100, however once puberty begins (typically age 11), referrals accelerate dramatically. Since 2010, girls aged between 12 and 17 have made up 86 per cent of all referrals. In 2021/22, this age group made up 90 per cent of all referrals.189Gender Identity Development Service, Number of referrals to GIDS. As aforementioned, all research in this space is limited, but Dr Cass notes there is a particular lack of data in this largest subgroup. Long-term studies and substantial research into the effectiveness of treatment options for this group are also difficult due to the fact this caseload is not yet in their mid-20s, when gender expression is more likely to be settled.190The Cass Review, pg.36. Puberty is a vulnerable period for young people, but arguably more so for girls, for the sexualisation of the female body is prevalent. Changing body shapes, body rejection and general body dysmorphia is much more common in girls.191S.Schneider, A.Baillie, J.Hudson et al, Measurement Invariance of a Body Dysmorphic Disorder Symptom Questionnaire Across Sex: The Body Image Questionnaire–Child and Adolescent Version, Assessment. 2018 Dec;25(8):1026-1035. https://pubmed.ncbi.nlm.nih.gov/27866170/ In 2018, then Equalities Minister, Penny Mordaunt, ordered an investigation into why a larger proportion of girls were experiencing gender distress, but the inquiry was never concluded.192G.Hurst, ‘Minister Penny Mordaunt orders research into rise of gender referrals for girls’ The Times, 17 September 2018. https://www.thetimes.co.uk/article/research-into-rise-of-girl-gender-referrals-w6b5v6fx5
6.2 Looked after children
Looked after children (LAC) is a term introduced by the Children Act 1989 to describe children in the care of their local authority, including those living with their biological family but subject to care orders.193Children Act 1989, Part III, Duties of local authorities in relation to children looked after by them. https://www.legislation.gov.uk/ukpga/1989/41/part/III/crossheading/duties-of-local-authorities-in-relation-to-children-looked-after-by-them A study published in 2019 (which reviewed 185 children referred to GIDS between 2009 and 2011), found that LAC represented 4.9 per cent of the cohort. At the time, LAC represented only 0.58 per cent of the population. In addition, adopted children represented 3.8 per cent of referrals, despite representing only 0.40 per cent of the overall under 18 population in England.194T.Matthews, V.Holt, D.Griksaitis et al, Gender Dysphoria in looked- after and adopted young people in a gender identity development service, Clinical Child Psychology and Psychiatry, Volume 24, Issue 1, August 2018. https://journals.sagepub.com/doi/full/10.1177/1359104518791657 There was not a statistically significant difference in biological sex nor age at the point of referral in this subgroup, however the insufficiency of the sample size is a possible limitation of this study. It is important to note that the mental health of LAC and adopted children is statistically much poorer than that of the overall child population. NICE notes that looked after children are four to five times more likely to experience mental health difficulties compared to their peers.195National Institute for Health and Care Excellence, Looked after children and young people: statement 5 https://www.nice.org.uk/about/nice-communities/social-care/tailored-resources/lacyp/statement-5
6.3 Children with autism
It is well documented that children with autism are an over-represented subgroup within the current caseload. The Interim Cass Report notes that approximately one third of children referred have autism.196The Cass Review, pg.32. Furthermore, a 2015 study of 166 young people from GIDS found that 54.2 per cent of young people scored in the autistic range having undertaken the Social Responsiveness Scale (SRS), a common quantitative measure designed to screen for the presence of an Autism Spectrum Disorder (ASD) condition.197E.Skagerberg, D.Di Ceglie & P.Carmichael, Brief Report: Autistic Features in Children and Adolescents with Gender Dysphoria, J Autism Dev Disord. 2015 Aug;45(8):2628-32. https://pubmed.ncbi.nlm.nih.gov/25772537/ Not all of these young people had been previously diagnosed with ASD, and the study notes that ‘based on clinical experience’ many referrers did not mention autistic traits when referring children. There is limited research on the link between ASD and gender distress in children. Some research suggests that isolation experienced as a result of poor understandings of social relationships can cause children to feel aversion to their own sex.198A.V.D.Miesen, H.Hurley & A.D.Vries, Gender dysphoria and autism spectrum disorder: A narrative review, Int Rev Psychiatry. 2016;28(1):70-80. https://pubmed.ncbi.nlm.nih.gov/26753812/ Autistic children are more likely to exhibit obsessive interests, and preoccupations, which can lead to obsessional interests with regard to gender.199Ibid.
6.4 Children questioning their sexuality
A further subgroup among the current caseload is the number of children questioning their sexuality. The Cass Interim Report notes that adolescence is often the time when sexuality and gender is explored, before young people settle into a more fixed identity.200The Cass Review, pg.27. In 2020, young people between 16-24 were the most likely group to identify as lesbian, gay or bisexual (LGB) – with 8 per cent falling into this category. This is a trend that has increased since 2014.201Office for National Statistics, Sexual Orientation, UK: 2020. https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/sexuality/bulletins/sexualidentityuk/2020 Research demonstrates that gender variant behaviour is associated with both gender dysphoria and sexual orientation. There is a strong correlation between early gender non-conforming behaviour and homosexuality. Girls who prefer ‘masculine’ activities are more likely to become lesbian, and boys who prefer ‘feminine’ activities are more likely to become gay.202L.Gu, K.Kung & M.Hines, Childhood gender-typed behavior and adolescent sexual orientation: A longitudinal population-based study, 2017 Apr;53(4):764-777. https://www.repository.cam.ac.uk/handle/1810/262671 A high proportion of gender-distressed children grow up to become gay, not transgender. A 2021 study of natal boys with GID (presenting at an average age of seven) demonstrated that 47.2 per cent were same-sex attracted when followed up 13 years later, regardless of whether they had transitioned.203D.Singh, S.Bradley & K.Zucker, A Follow-Up Study of Boys With Gender Identity Disorder, Front Psychiatry. 2021; 12: 632784. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8039393/ Gender non-conformity in childhood is much more of a predictor of LGB orientation in adulthood than transgenderism. GIDS Director, Dr Polly Carmichael, said during a 2015 article for The Guardian that prepubescent children with gender dysphoria will have a different outcome in adulthood: “The most common would be one around sexuality, rather than gender identity.” In her experience, they are more likely to be LGB than transgender.”204J.Kleeman, Transgender children: ‘This is who he is – I have to respect that’ The Guardian, 12 September 2015. https://www.theguardian.com/society/2015/sep/12/transgender-children-have-to-respect-who-he-is
6.5 Poor mental health: a symptom or cause of gender distress?
Poor adolescent mental health is on the rise more generally.205NHS Digital, Mental Health of Children and Young People in England 2021 – wave 2 follow up to the 2017 survey, 30 September 2021. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2021-follow-up-to-the-2017-survey#highlights However, there is an especially strong link between poor mental health and gender distress. In 2021, the NHS reported that 39.2 per cent of six-16-year-olds had experienced a deterioration in their mental health since 2017. In this period, rates of probable mental disorders in children increased from one in nine to one in six.206NHS Digital, Mental Health of Children and Young People in England 2021 – wave 2 follow up to the 2017 survey. Furthermore, all of the subgroups in the current caseload described above are statistically more vulnerable to poor mental health than the average adolescent population. The Cass Interim Report notes there is limited evidence of routine mental health assessment taking place within GIDS, thus it is difficult to decipher more granular trends within this presentation.207The Cass Review, pg.17. The correlation between rising referral rates for gender distress and rising poor adolescent mental health needs to be better understood, and especially, whether poor mental health is a symptom or a cause of gender distress. In some cases, persistent and unresolved gender distress may cause a child significant mental health issues. This may well be because of the distress caused by the dysphoria but also because of bullying or social stigma. Until there is further empirical evidence to understand the causal link between the two conditions, any treatment path should be cautious about the idea that solving gender distress will solve a child’s other mental health problems, and vice versa.
Next chapter7. How are schools dealing with this issue?
In December 2022, Policy Exchange submitted over 300 Freedom of Information (FOI) requests to a selection of maintained secondary schools and academies in England.208Under the Freedom of Information Act 2000, organisations have 20 working days to respond to a request. Schools that responded after 15 February 2023 have not been counted. The purpose of this research was to determine how well a sample of schools were upholding the basic safeguarding principles explained earlier. The questions asked assessed both how well schools were safeguarding gender-distressed children and their peers, as well as what they were teaching about sex and gender in RSHE. This chapter will document the results of this survey, highlighting trends and notable responses.
Recent polling by Policy Exchange found that one in four young people (18-20) identify as LGBT, which suggests that many school leavers are exploring their identity at school.209E.Kaufmann, The Political Culture of Young Britain, Policy Exchange, 19 November 2022. https://policyexchange.org.uk/wp-content/uploads/2022/11/The-Political-Culture-of-Young-Britain.pdf The challenge facing schools is clear. The gender affirmation of children in isolated clinical settings requires scrutiny, but the implications of such policies have much wider implications on schools, which must manage this influx of alternative identities while still safeguarding and respecting the needs and rights of all children and staff. Related to how schools are coping with children presenting with gender distress is the appropriateness of current RSHE, and the impact of this teaching on children’s beliefs about their own sex and gender.
In total we sent FOI requests to 304 schools, representative of the number of schools in every Local Authority (LA) in England. Due to the size of the sample, schools per LA were selected at random. Of 304 requests, 56 special schools were excluded, three requests were refused, 91 did not respond, and 154 responded – either fully or in part – to the questions asked. We excluded special schools on the basis that many of the issues raised are not applicable or relevant to these schools. In the findings, where a school provided no information to a particular question, their response was categorised as such but is not included below. Where a clear answer to a question could not be discerned, a school’s answer is categorised under ‘insufficient detail provided.’
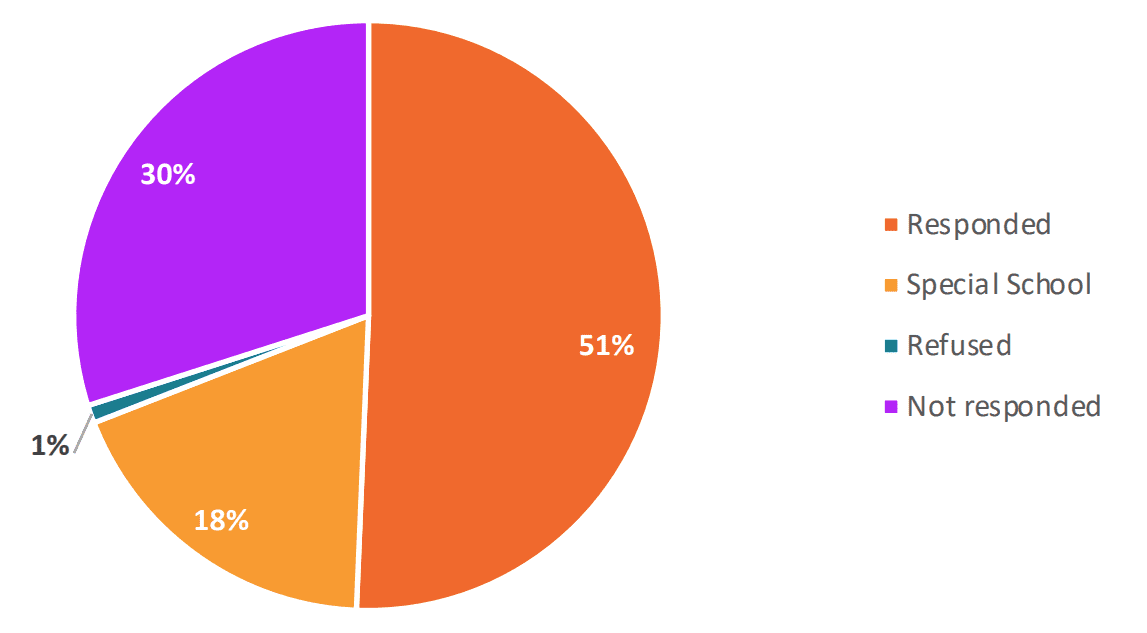
| Responded | 154 | 51% |
| Refused | 3 | 1% |
| Special schools | 56 | 18% |
| Not responded | 91 | 30% |
| Total | 304 | 100% |
| What we asked schools |
We made clear to schools that in the questions above, ‘sex’ refers to a child’s biological sex, whereas gender refers to a perceived gender identity that a person may consider they have, that may or may not match their biological sex. We also asked schools to share any relevant curriculum resources or policies relating to the matters in question. |
7.1 To what extent are schools involving parents?
Overwhelmingly, our results show that schools are not reliably informing parents as soon as a pupil expresses the wish to change gender. While many schools stated that they would encourage students to talk to their parents, there is a clear consensus that schools should be wholly led by the feelings and wishes of the child.
Only 28 per cent of parents are reliably informed when a child expresses feelings of gender-distress at school.
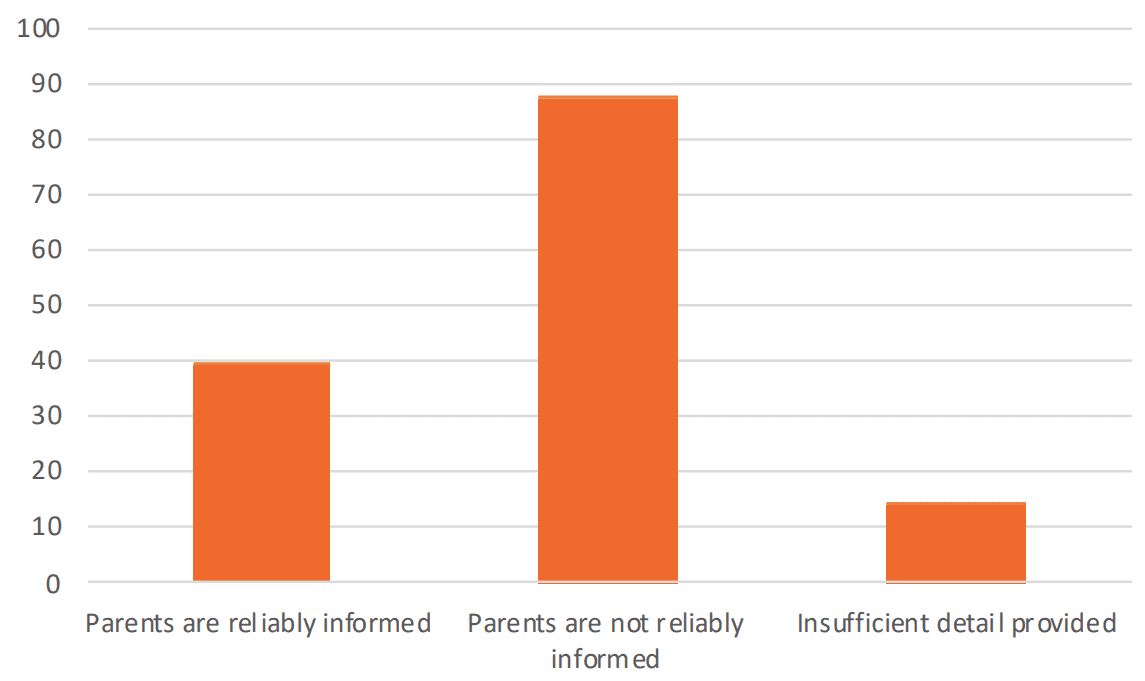
| Parents are reliably informed | 39 | 28% |
| Parents are not reliably informed | 87 | 62% |
| Insufficient detail provided | 14 | 10% |
|
Number of schools who answered the question: 140/154 |
||
As per the example below, one school mistakenly referenced the Equality Act 2010 (EA) as justification for not informing parents of a pupil’s wish to change gender. The EA is concerned with protecting people from discrimination. There is nothing in the legislation regarding parental consent in relation to the protected characteristic of gender reassignment. If a person possesses a protected characteristic, they cannot be discriminated against for it. Informing a parent of safeguarding issue relating to their child does not interfere with this legal protection.
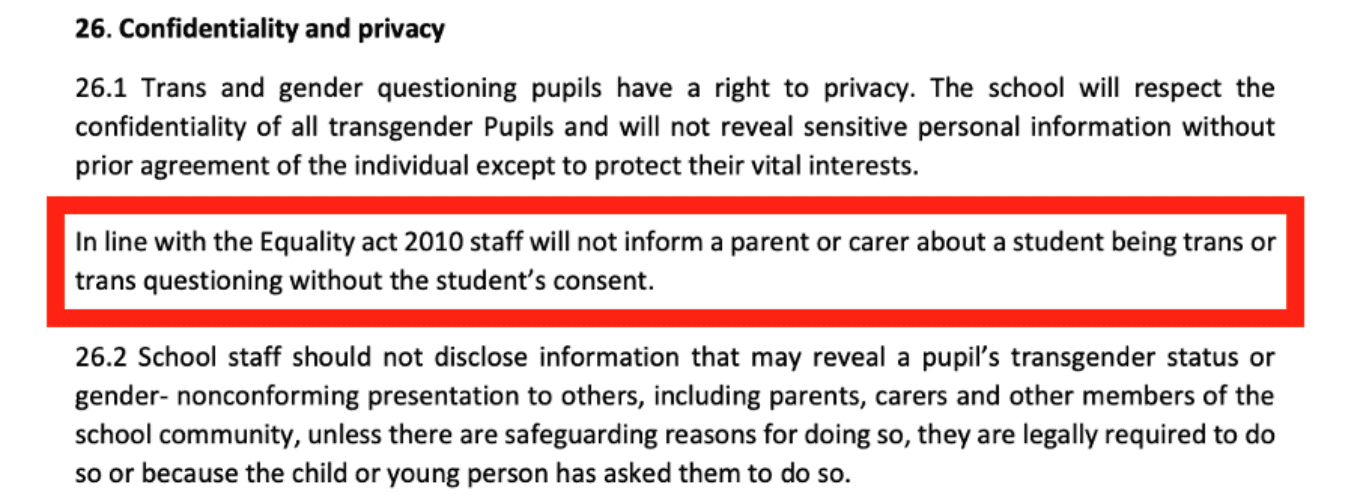
Part of one school’s specific Transgender Guidance Policy.
The emphasis placed on the wishes and innate feelings of child above parental consent is clear in the findings. One school in particular stressed that they would generally inform parents, but would do so out of courtesy, rather than mandatory safeguarding protocol.

One school responds that they inform parents as a matter of courtesy.
One school stated that it would be unlawful to share information about a gender-distressed child with their parents on the basis of the Data Protection Act 2018. This is a complete misunderstanding of the law. As explored earlier, all mandatory safeguarding documents applicable to schools, and the Act itself is clear that GDPR does not prevent the sharing of information for the purposes of keeping children safe and preventing them from harm.210KCSIE, pg.18, WTKCS, pg.19, Data Protection Act 2018, Schedule 12, Safeguarding of children and of individuals at risk. https://www.legislation.gov.uk/ukpga/2018/12/schedule/8/crossheading/safeguarding-of-children-and-of-individuals-at-risk

Several schools referred to their local authority’s guidance on how schools in the LA should deal with this issue. A number of schools responded that while they did not hold specific policies, or have experience of dealing with gender-distressed pupils, they would look to their local authority for guidance when they needed to.
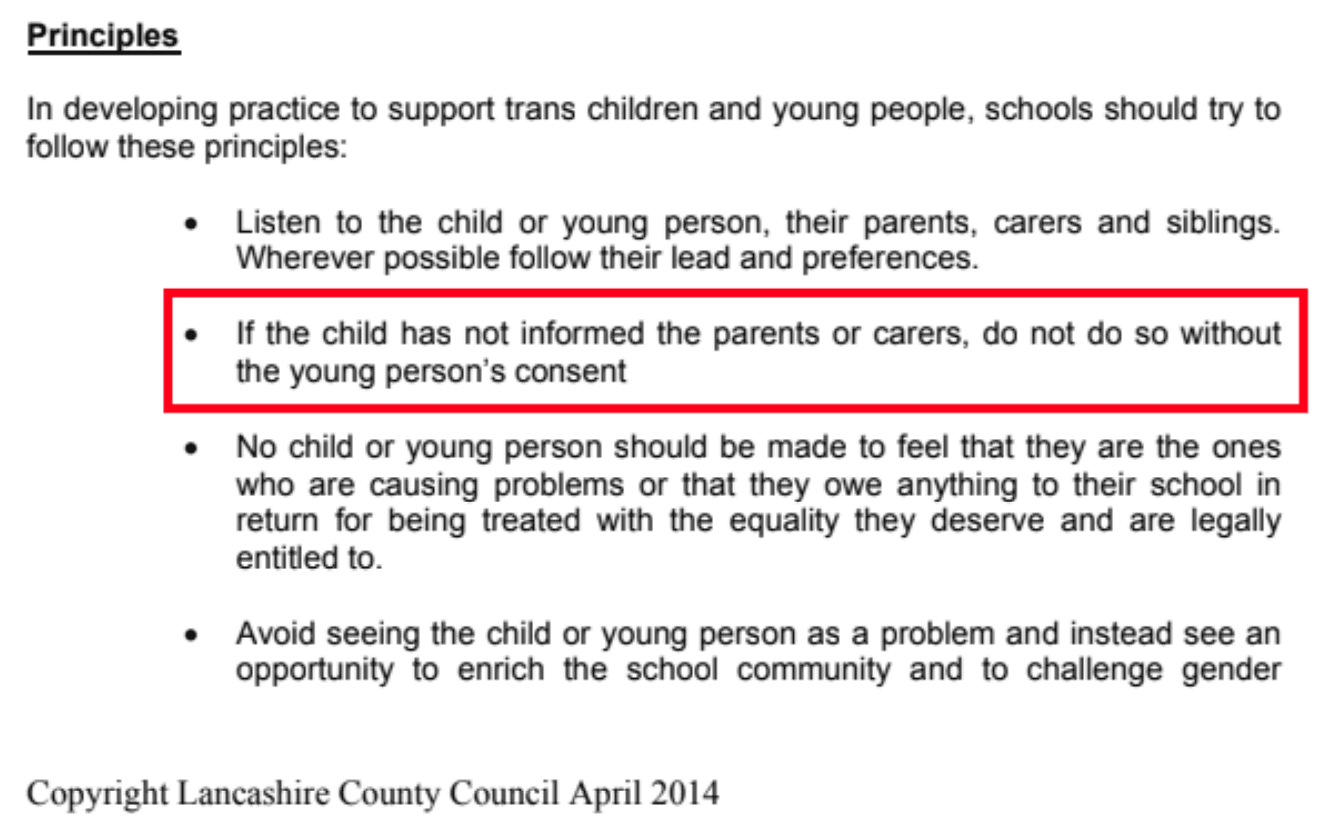
Lancashire County Council’s ‘Transgender Guidance’, last updated in 2014.
One school based in Cornwall referenced Cornwall Council’s Transgender Guidance, which was published in 2015.211Cornwall Council, Cornwall Schools Transgender Guidance, last updated: 23 November 2022. http://www.lgbtqyouthcornwall.co.uk/images/TransGuidance/Transgender_Guidance_booklet%20a4.pdf The guidance was produced in conjunction with Intercom Trust, an LGBT charity based in the South West, Devon & Cornwall Police and Cornwall Council. It is not clear why the police were involved in creating the guidance, because nothing in its content relates to crime or police matters. Despite this, Cornwall Police Constable and the forces’ Diversity Officer Toby Best, who co-wrote the guidance, was awarded the Chief Superintendent’s Commendation for his contribution to the document.212Devon & Cornwall Police, West Cornwall police officers recognised at awards ceremony, 22nd October 2014. https://www.falmouthpacket.co.uk/news/11551914.west-cornwall-police-officers-recognised-at-awards-ceremony/
Relating to the role of parents, the guidance appears to suggest that informing a parent of a child’s transition without their permission could constitute discrimination against transgender people:
‘It must be recognised that people have their own prejudices. A parent or guardian may not always be the most supportive or appropriate person to assist the young person through transitioning. It may not be necessary for a parent or guardian to provide permission for a Trans pupil or student to take steps to transition as there may be issues raised of Fraser competence if parents will not consent.’213Cornwall Council, Cornwall Schools Transgender Guidance, pg.18.
Again, this is incorrect. The legal protections accorded to the protected characteristic of gender reassignment mean a person possessing this characteristic cannot be discriminated against. A parent unsupportive of their child’s wish to transition does not automatically constitute discrimination. Parents are not duty-bearers under the Equality Act.214Equality Act 2010, Part 2, Chapter 2. https://www.legislation.gov.uk/ukpga/2010/15/part/2/chapter/2
‘Schools Transgender Guidance’ produced by the Intercom Trust, Devon and Cornwall Police and Cornwall County Council.215Cornwall Council, Cornwall Schools Transgender Guidance, pg.7.
One school’s specific transgender guidance policy.
Some schools suggest that informing parents of their child’s gender distress would breach a child’s confidentiality. This is in direct contradiction to safeguarding standards. As aforementioned, KCSIE explicitly states that confidentiality of any kind should never be promised to a child.
Another school’s transgender policy suggests that informing parents of a child’s gender distress would be in breach of confidentiality.
7.2 To what extent are schools involving safeguarding or medical professionals?
A much smaller – but still concerning – number of schools answered that they would not involve a safeguarding or medical professional if a child expressed gender distress. A number of schools stated that they would assess who would be consulted on a case-by-case basis. We also asked schools to list the relevant job roles they consult when or if this matter arises. There were some encouraging examples of multi-agency working, where the default position was for a DSL, local Child and Adolescent Mental Health Services (CAMHS) and parents to work together.
While 54 per cent of schools stated that they would inform a safeguarding and/or medical practitioner when a pupil disclosed gender distress, 33 per cent said they would not automatically do this.
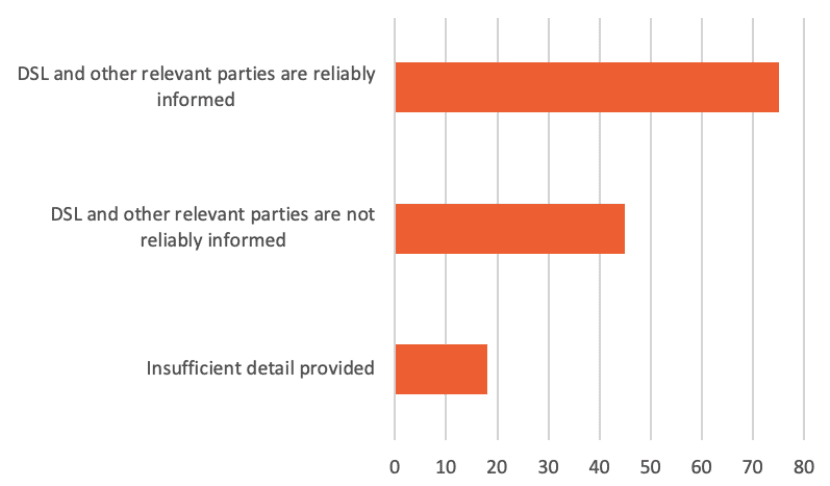
| DSL and other relevant parties are reliably informed | 75 | 54% |
| DSL and other relevant parties are not reliably informed | 45 | 33% |
| Insufficient detail provided | 18 | 13% |
| Total number of schools that provided information: 138/154 | ||
A small number of schools explained that they would inform an LGBT officer instead of a DSL or medical practitioner. While raising awareness of preventing discrimination in schools is positive, when a child discloses feelings of gender distress, at a minimum, a DSL or medical practitioner should be informed.
![]()
In response to this question, a school stated that they have ‘trained skilled staff who wear rainbow lanyards’, but not a safeguarding professional, parent or medical practitioner.
7.3 To what extent are schools operating policies of gender self-identification?
Gender self-identification (self-ID) refers to the process of a person identifying as their preferred gender without any external requirements, because the person’s own innate feeling about their sense of self as male or female is considered necessary validation. While some schools operate self-identification – but with parental consent – only a very small proportion of schools stated that they did not operate some form of pupil self-identification on their premises.
Many schools state that parental consent would be needed to change a child’s name on their information management system. A school’s support for self-ID without parental consent means there may well be instances where the first time a parent is informed of their child’s transition is on a letter home, where the child’s new name is referenced.
Four in ten schools operate self-identification for gender identity: in other words, they consider the gender of a child to be the gender that the child declares it to be.
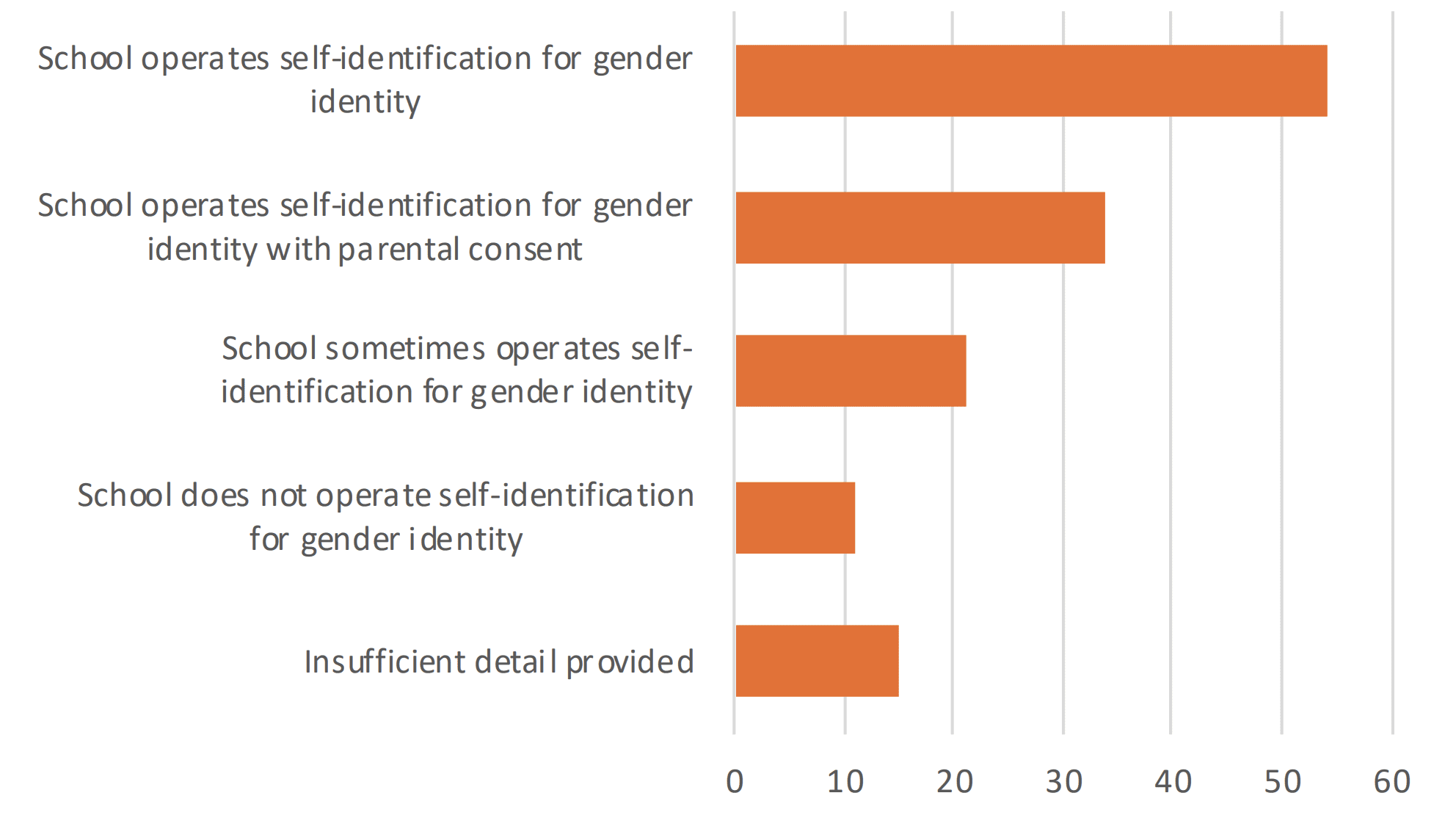
| School operates self-identification for gender identity | 54 | 40% |
| School operates self-identification for gender identity with parental consent | 34 | 25% |
| School sometimes operates self-identification for gender identity | 21 | 16% |
| School does not operate self-identification for gender identity | 11 | 8% |
| Insufficient detail provided | 15 | 11% |
| Number of schools that provided information: 135/154 | ||
One school’s approach to self-identification.

Another school’s approach to self-identification.
7.4 How are other children impacted by schools’ approaches to gender-distressed children?
We asked schools for their policies on three elements relating to single sex provision: toilets, changing rooms and sports. Overall, schools were more likely to retain single sex provision in all three elements. However, schools were significantly more likely to allow a socially transitioned child to partake in opposite sex sports, than allow them to use opposite sex toilets or changing rooms. Where a school stated that they provide gender neutral facilities but did not clarify whether they also maintain single-sex facilities, the answer has been categorised under ‘insufficient detail provided’.
At least 28 per cent of schools do not maintain single-sex toilets, while 35 per cent of schools ensure toilets are single-sex.
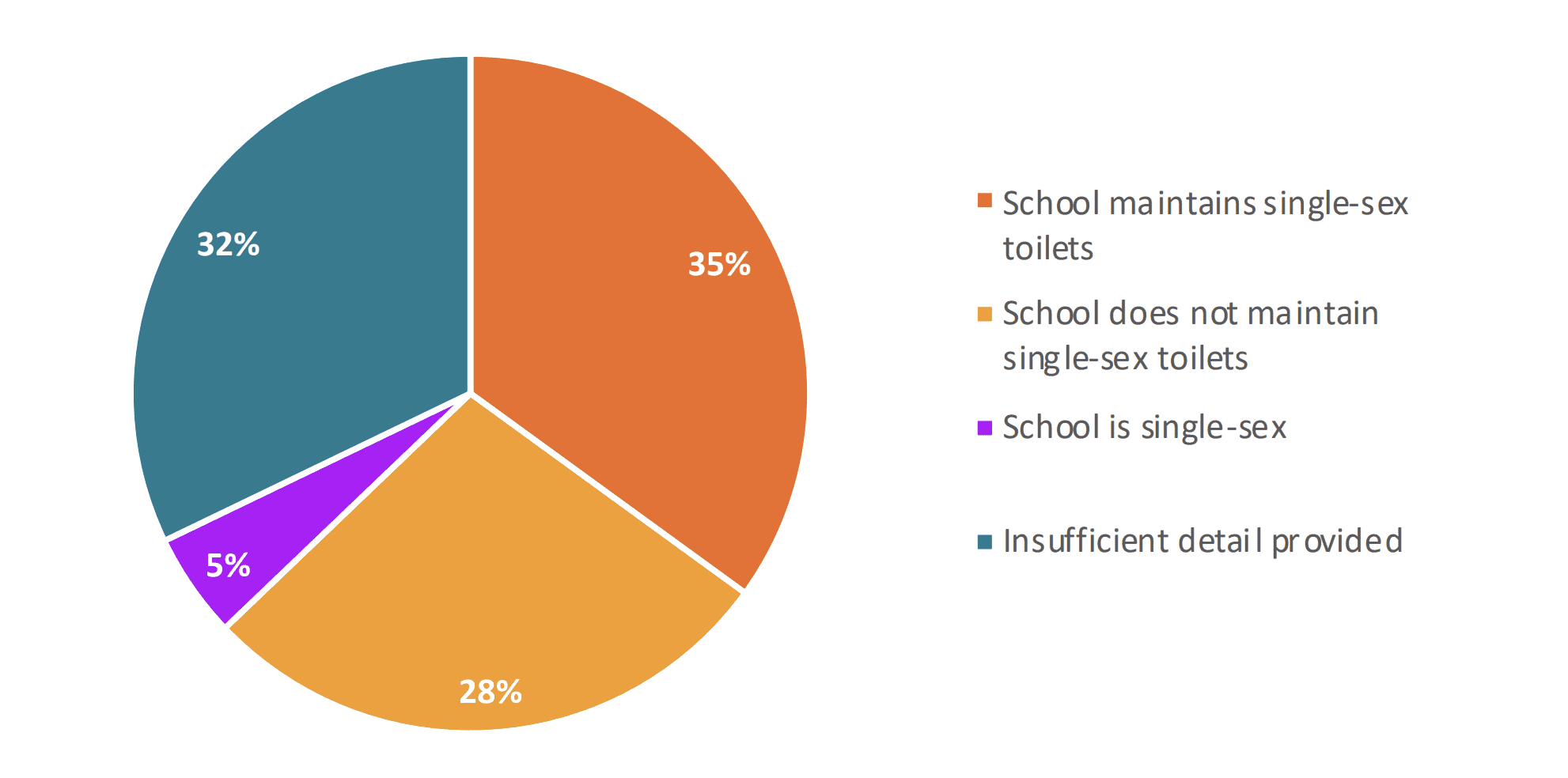
| School maintains single-sex toilets | 49 | 35% |
| School does not maintain single-sex toilets | 39 | 28% |
| School is single-sex | 7 | 5% |
| Insufficient detail provided | 45 | 32% |
| Number of schools that provided information: 140/154 | ||
At least 19 per cent of schools do not maintain single-sex changing rooms, while 40 per cent of schools ensure changing rooms remain single-sex.
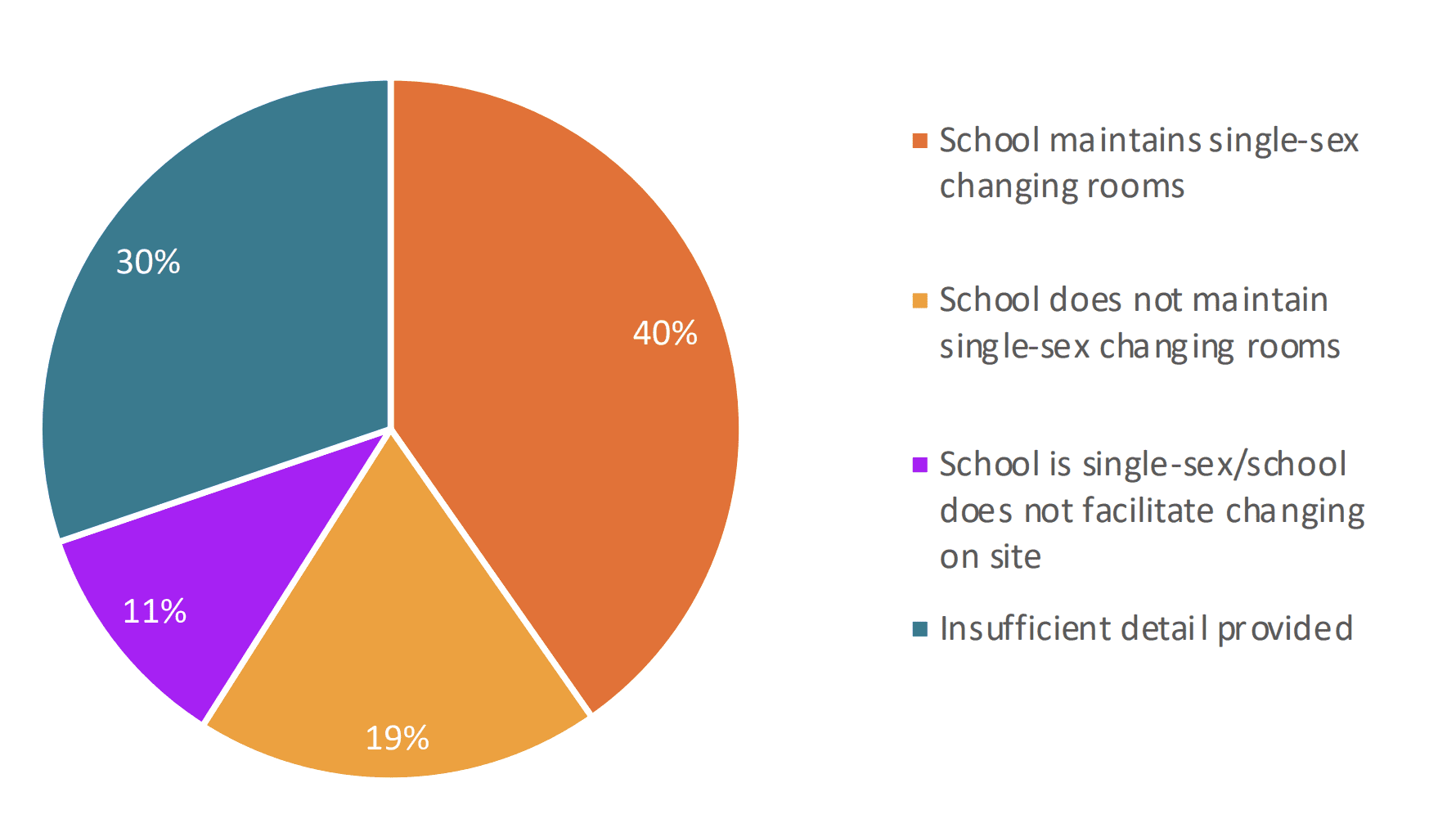
| School maintains single-sex changing rooms | 56 | 40% |
| School does not maintain single-sex changing rooms | 26 | 19% |
| School is single-sex/school does not facilitate changing on site | 15 | 11% |
| Insufficient detail provided | 42 | 30% |
| Number of schools that provided information: 139/154 | ||
At least 60 per cent of schools are not maintaining single-sex sports. Only six per cent of schools require gender-distressed children to participate in sports of their biological sex.
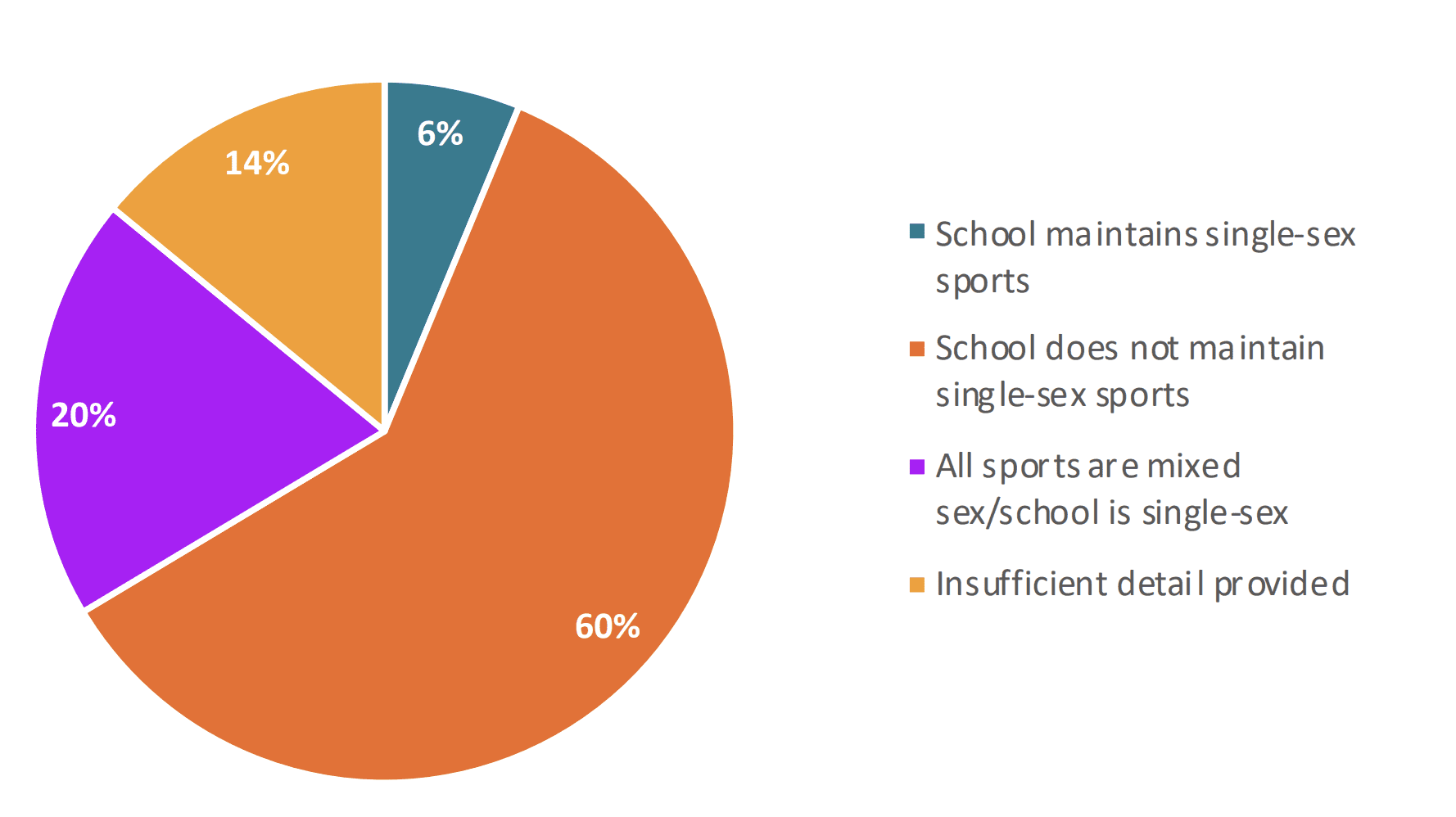
| School maintains single-sex sports | 8 | 6% |
| School does not maintain single-sex sports | 77 | 60% |
| All sports are mixed sex/school is single-sex | 25 | 20% |
| Insufficient detail provided | 18 | 14% |
| Number of schools that provided information: 128/154 | ||
A number of schools responded that while they would not permit a child to use the facilities of the opposite sex, alternative facilities would be provided if the child felt uncomfortable using the facilities of their biological sex. A small number of secondary schools stated that all toilets were unisex and there were no same-sex facilities. This is a potential breach of the law. Under The School Premises (England) Regulations 2012, schools are legally required to provide single-sex toilets and washing facilities for children over eight, ‘except where the toilet facility is provided in a room that can be secured from the inside and that is intended for use by one pupil at a time.’216The School Premises (England) Regulations 2012, UK Statutory Instruments, 2012 No. 1943, Regulation 4.https://www.legislation.gov.uk/uksi/2012/1943/regulation/4/made If a school has made all previously sex-separated facilities unisex – without fulfilling this requirement – they are in breach of the law.
One school that permits students to use facilities of the opposite sex.
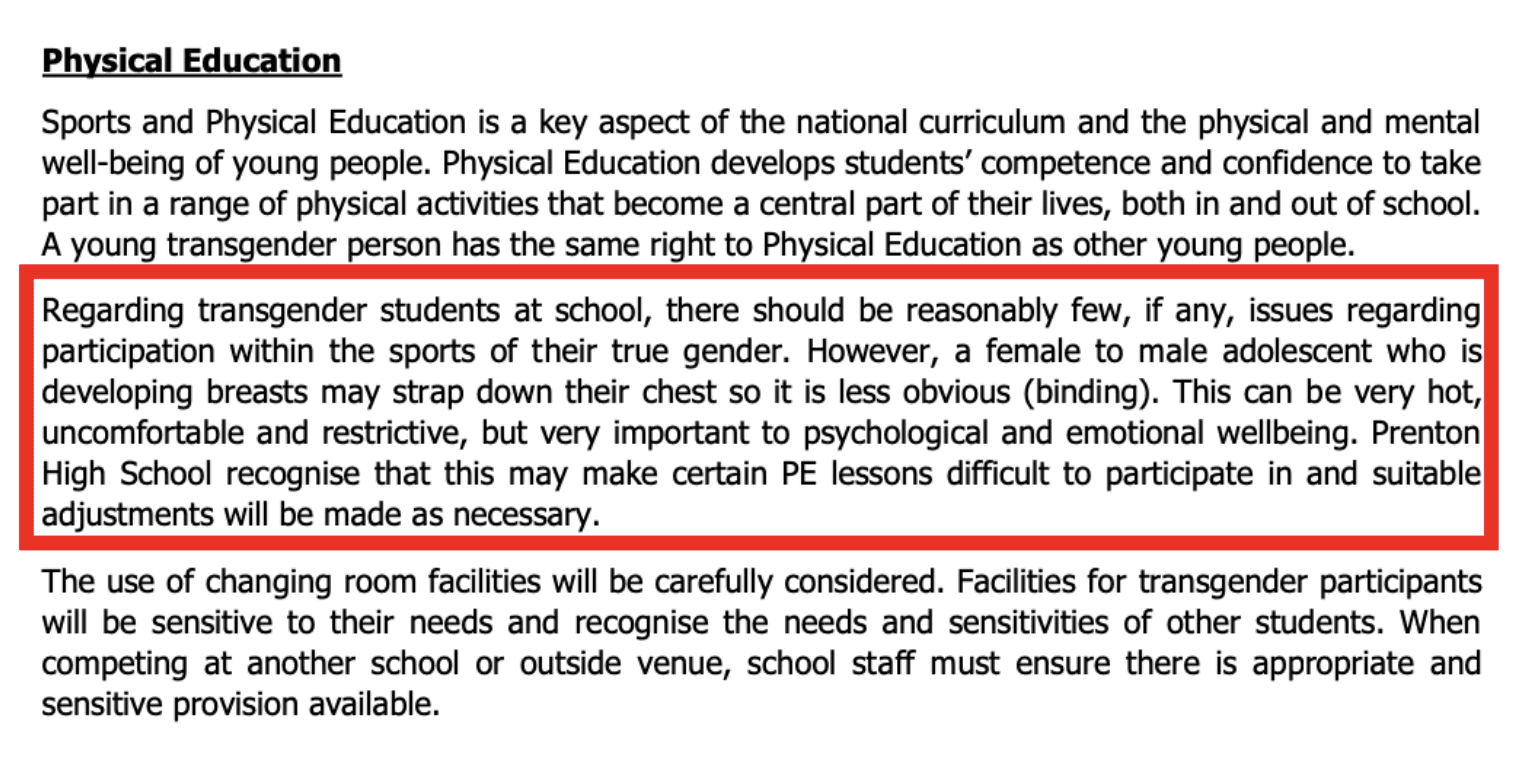
The physical education section of one school’s transgender guidance.
We also asked schools whether they required other children to refer to a socially transitioned child by their new name and pronouns.
69 per cent of schools require other children to affirm a gender-distressed child’s new identity. Only 13 per cent of schools do not require pupils to participate in the social transition of another pupil.
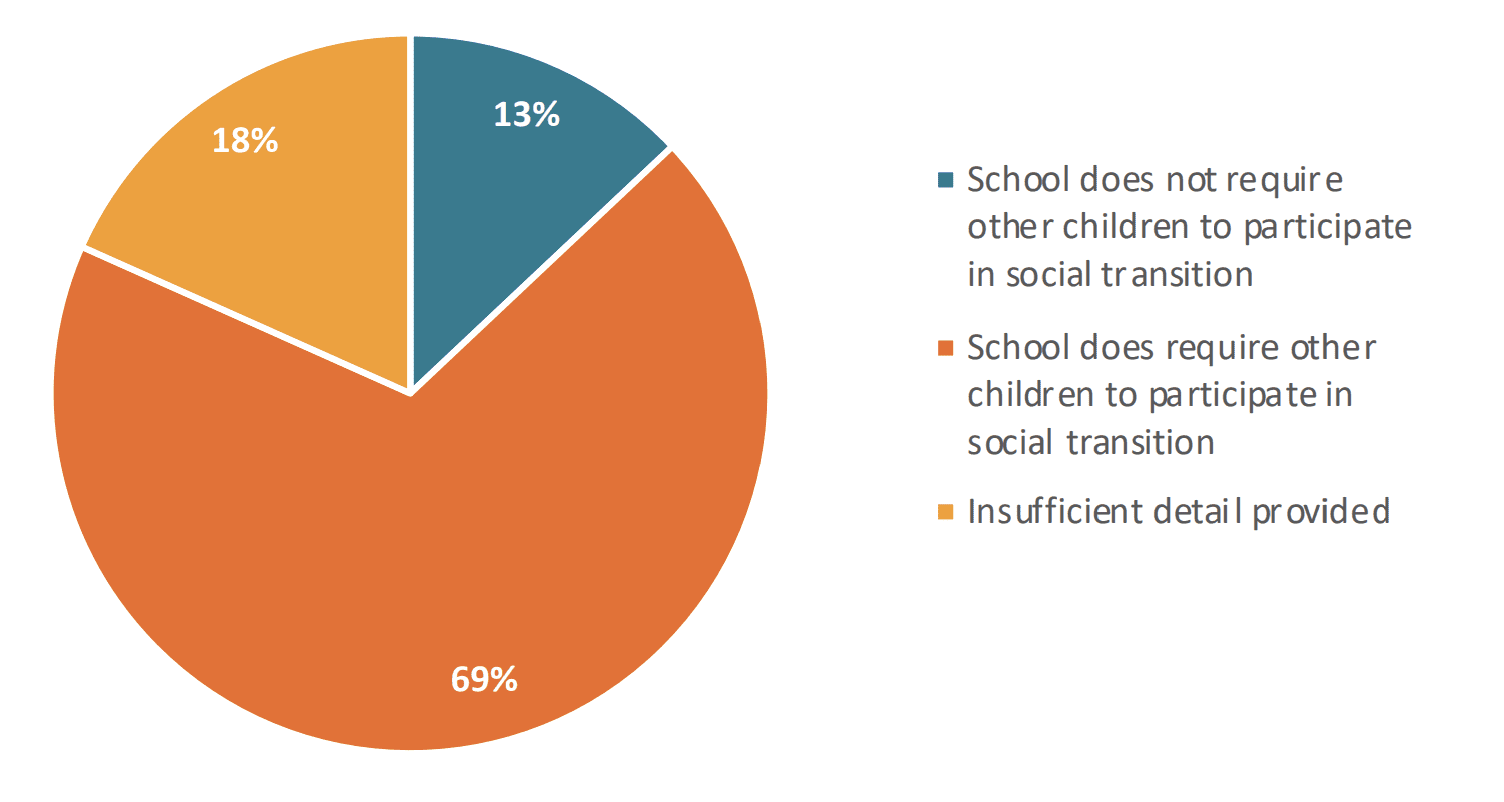
| School does not require other children to participate in social transition | 17 | 13% |
| School does require other children to participate in social transition | 90 | 69% |
| Insufficient detail provided | 24 | 18% |
| Number of schools that provided information: 131/154 | ||
A number of schools associated this question with transphobia or invoked their commitment to be inclusive, the implication being that if a school did not require other children to affirm a socially transitioned child’s new identity, this would be both transphobic of the school, or of the students who did not affirm the child.

One school’s direct response to the question.

Another school states: ‘student will be taught why its important to ensure they use the correct pronouns as a respectful and inclusive act.’
One school referenced the protected characteristic of gender reassignment under the Equality Act 2010 (EA) as justification as to why a child must affirm a child’s new identity. The EA prevents a person with the characteristic of gender reassignment being discriminated against. It does not require a child to be treated as if they were the opposite sex – there is no mention of preferred names or pronouns in the legislation.

In response to the question, one school stated that the protected characteristic of gender reassignment under the Equality Act 2010 means that a child’s new identity must be affirmed.
7.5 What are schools teaching on sex and gender?
We asked schools three questions related to teaching on gender identity. Firstly, we asked schools whether they teach a fundamental statement relating to gender identity beliefs. 72 per cent of schools informed us that they teach pupils that people have a gender identity that may be different from their biological sex. A much smaller number – 25 per cent of schools – teach that some people or children are born in the wrong body. Similarly, at least 30 per cent of schools teach their students that a person who self-identifies as a different gender should be treated as that gender in all circumstances, even if this doesn’t match their biological sex. We also asked schools to provide resources where possible.
72 per cent of schools teach the idea that people have a gender identity that may be different from their biological sex.
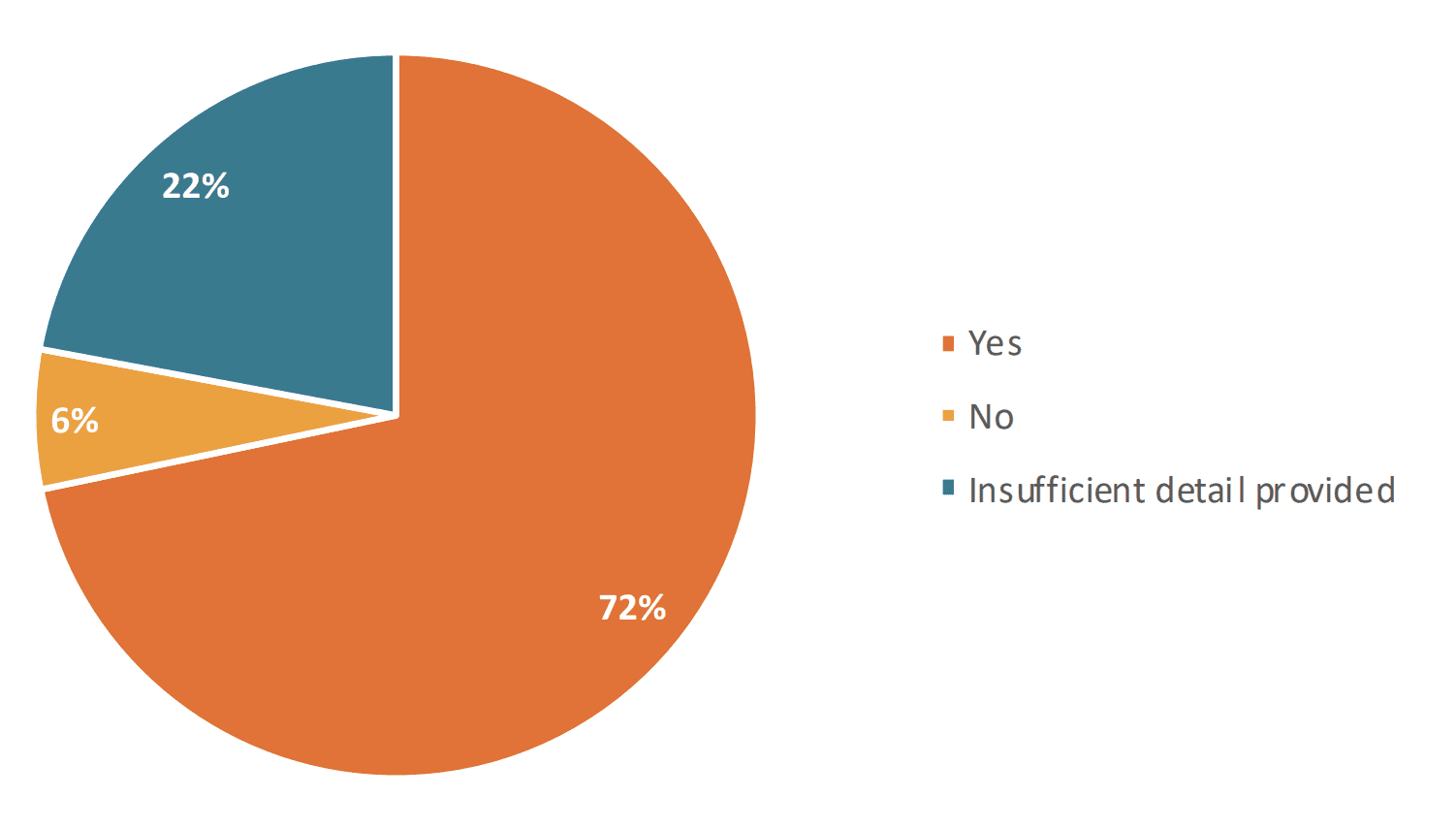
| Yes | 104 | 72% |
| No | 9 | 6% |
| Insufficient detail provided | 32 | 22% |
| Number of schools that provided information: 145/154 | ||
At least 25 per cent of schools teach the idea that some people or children ‘may be born in the wrong body.’
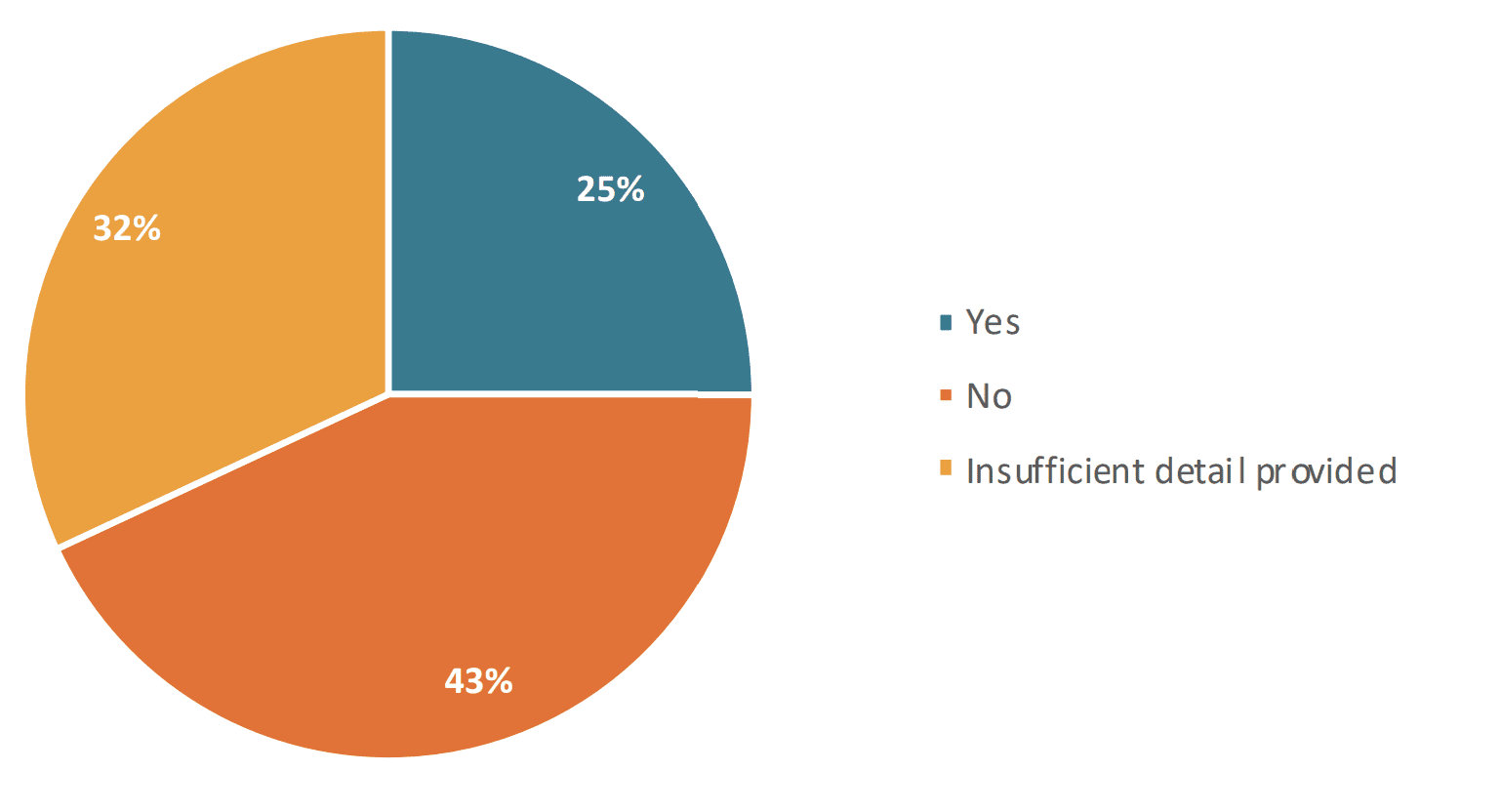
| Yes | 36 | 25% |
| No | 62 | 43% |
| Insufficient detail | 46 | 32% |
| Number of schools that provided information: 144/54 | ||
At least 30 per cent of schools teach pupils that a person who self-identifies as a man or a woman should be treated as a man or woman in all circumstances, even if this does not match their biological sex.
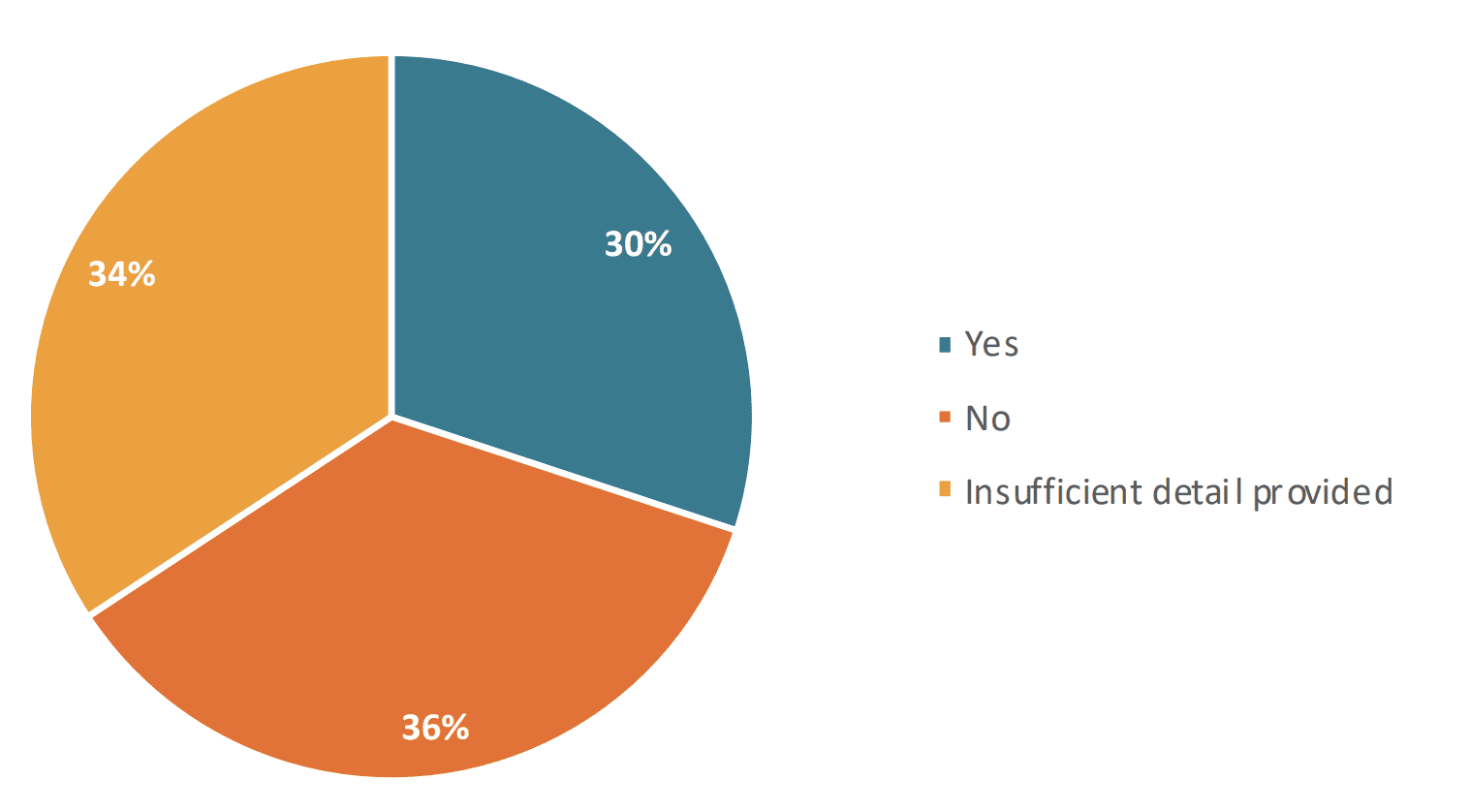
| Yes | 43 | 30% |
| No | 51 | 36% |
| Insufficient detail | 49 | 34% |
| Number of schools that provided information: 143/154 | ||
A number of resources are teaching pupils that there are more than just male and female gender identities. RSHE resources across several different schools ask children to define up to 15 different types of identity a person may feel they have.
The ‘Genderbread Person’ is a resource produced by ‘global justice initiative’ Hues. The Genderbread Person is a free downloadable ‘teaching tool for breaking down the big concept of gender down into bite-sized, digestible pieces.’217The Genderbread Person, Genderbread Person v4.0. https://www.genderbread.org This diagram featured in several curriculum resources. The Genderbread Person reduces a child’s identity to a number of highly contested beliefs, which again are not based in evidence.
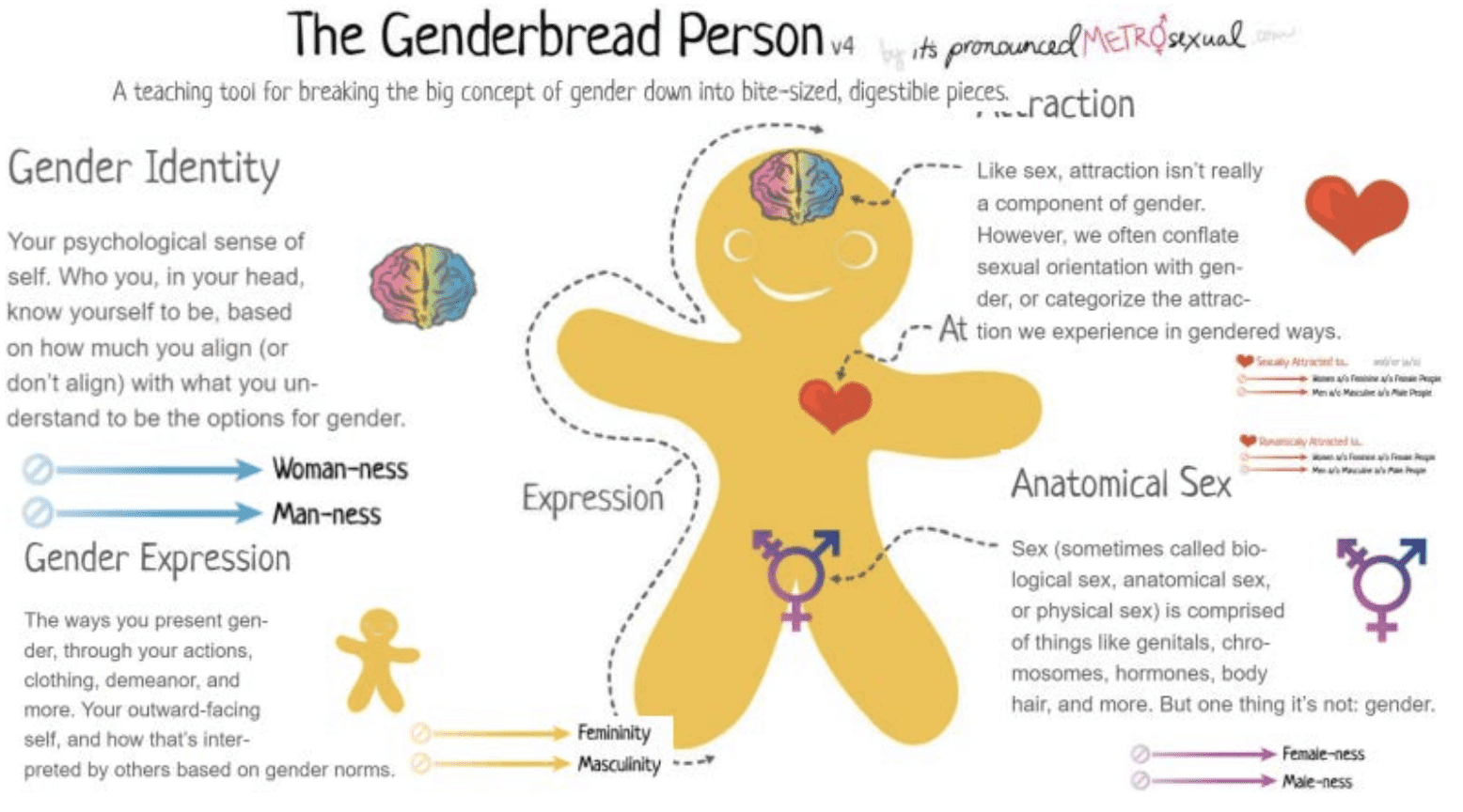
The Genderbread Person.
This idea was originally produced by comedian Sam Killermann, who wrote the accompanying article ‘Breaking through the binary: Gender explained using continuums’.218S.Killerman, Breaking through the Binary, The Genderbread Person. https://www.genderbread.org/wp-content/uploads/2017/02/Breaking-through-the-Binary-by-Sam-Killermann.pdf In this article, he suggests that childrens’ innate identities are based on heavily regressive and somewhat sexualised gender stereotypes.
Sam Killerman’s explanation of the Genderbread Person’s gender expression for children.
Again, this is in direct conflict with government guidance, which is clear: children who wear certain clothes or enjoy certain activities should not be encouraged to think they are the opposite sex.
‘Materials which suggest that non-conformity to gender stereotypes should be seen as synonymous with having a different gender identity should not be used and you should not work with external agencies or organisations that produce such material.’219Gov.UK, Plan your relationships, sex and health curriculum.
A school’s external resources for Year 8 (Aged 12-13) teaching children that gender is not binary.
One school’s description of gender identity.
The resource below outlines to pupils terms they should avoid, one of which is discussion relating to biological sex. It also implies that sex is not binary. Similarly, the Genderbread image above implies that biological sex exists on some kind of sliding scale. This is of course, incorrect. Sex is immutable and defined by chromosomal DNA.
In a class on gender identity and sexual orientation, a presentation informs students of terms which may be considered offensive.
One school teaches that children should be able to define at least five gender identities.
7.6 What sorts of external agencies are schools using?
We asked each school whether they had engaged with an external agency in delivering RSHE in the last 24 months. Over 50 per cent of schools stated that they had. The most common organisations named were:
- PSHE Association
- The Proud Trust
- Rainbow Flag Award
- Just Like Us
- Diversity Role Models
52 per cent of schools stated that they had used a provider (charity or commercial organisation) to provide lessons or resources on gender identity.
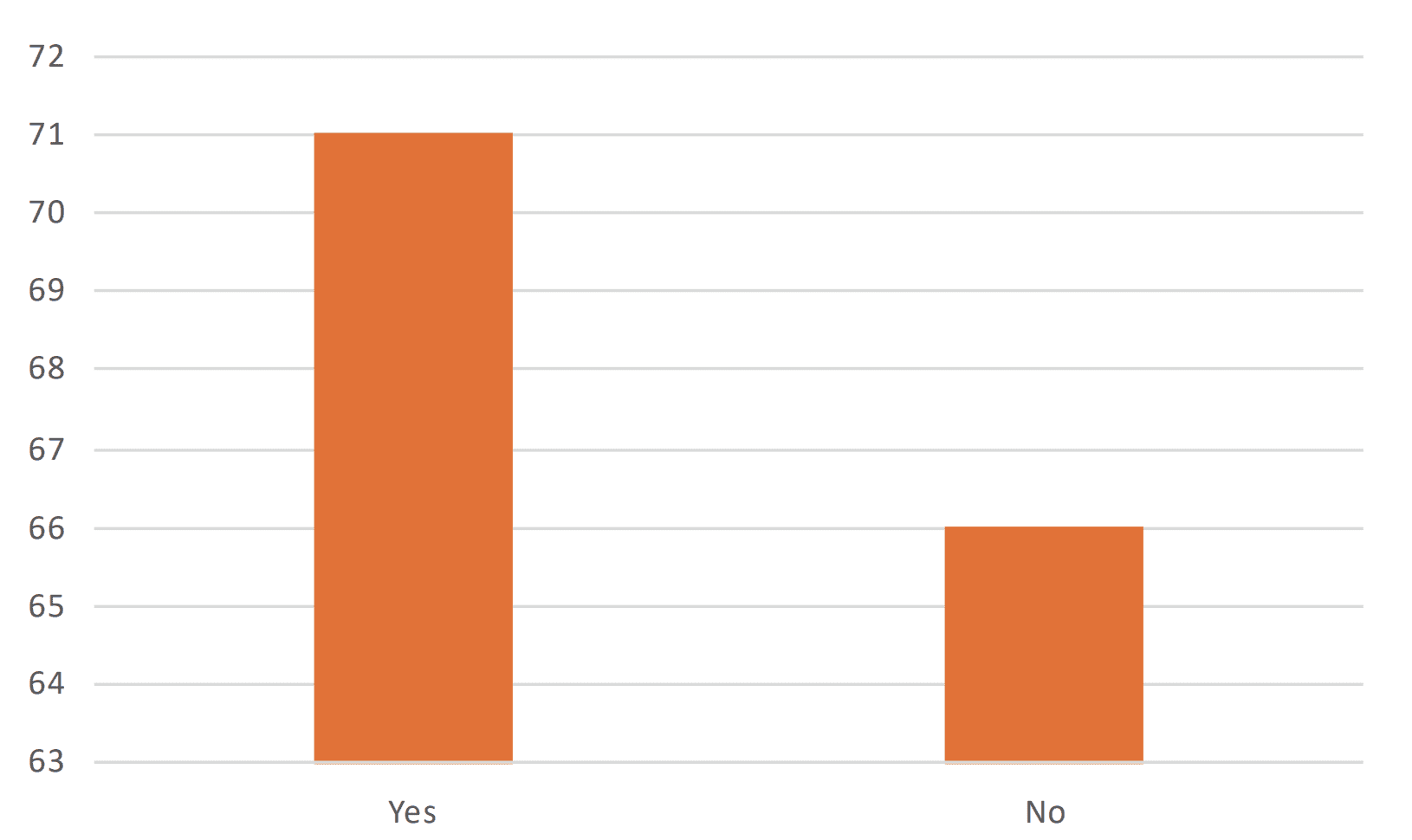
| Yes | 71 | 52% |
| No | 66 | 48% |
| Number of schools that provided information: 137/154 | ||
The Government has given large amounts of funding to several of the external agencies the schools we asked had worked with. This will be explored in chapter ten. Most of these agencies operate as umbrella organisations with multiple aims, such as equality, anti-bullying or LGBT inclusion aims. It is under this guise that many of these agencies are expressing overtly political and partisan views.
Next chapter8. What are the implications of current practice on safeguarding?
As demonstrated, the affirmative approach towards treating children with gender distress is common within both clinical and educational settings within the UK. While social transition may appear to be a harmless and superficial expression of identity, the medical journey it sets so many children on is not. It is important to understand that safeguarding is only as effective as those who implement it. Safeguarding principles regarding gender-distressed children require professionals working with children to respect the fact that gender-distress is a safeguarding issue. It is clear that many schools do not regard gender-distress and its associated pathway as a safeguarding issue. Subsequently, the implications of current practice on safeguarding principles is substantial.
8.1 Social transition is an active intervention
Childhood and adolescence are common ages to explore identity. This has led to the sense that if a child expresses discomfort with their sex, adopting the style and attributes of the opposite sex is a relatively harmless and neutral act. The affirmative approach might consider the fact that just as a teenager might identify as a ‘goth’ or an ‘emo’, a child wishing to identify as the opposite gender is a normal expression of a possibly transient identity. In this way, social transition is not generally considered to be a medical intervention, not least because it does not generally take place in health settings.
Nonetheless, social transition is an active medical intervention. The Cass Interim Report states that in and of itself, social transition ‘may have significant effects on the child or young person in terms of their psychological functioning.’220The Cass Review, pg. 62. The fact that social transition is a medical treatment is not in and of itself an objection to it. As aforementioned, for a small number of children, social transition and the subsequent treatment path it leads to may be appropriate. However, the Interim Report is clear that it is simply impossible to know which children within the current caseload will go onto inhabit stable transgender identities as adults. This report argues that is that it is particularly impossible for schools to know this. As such, the medical intervention of social transition comes with serious risks – and certainly has no place within an education setting.
The long term effects of social transition are not known, and there are reasons to be sceptical about its success as a treatment for gender dysphoria. The NHS notes that ‘the current evidence base is insufficient to predict the long-term outcomes of complete gender-role transition during early childhood.’221NHS England, NHS Standard Contract for Gender Identity Development Service for Children and Adolescents, Schedule 2, The Services, pg.5. https://www.england.nhs.uk/wp-content/uploads/2017/04/gender-development-service-children-adolescents.pdf
Returning to the trend of persistence and desistance, studies indicate that the vast majority of children who do not socially transition find their gender dysphoria is resolved when followed up in adolescence or adulthood.222D.Singh, S.Bradley & K.Zucker, A Follow-Up Study of Boys With Gender Identity Disorder. Conversely, the rate of gender dysphoria persistence is much higher for children who do socially transition – social transition as a form of treatment may therefore be considered in some cases to be iatrogenic.223K.Zucker, Debate: Different strokes for different folks, Child and Adolescent Mental Health, Volume 25, Issue 1, 2019. https://acamh.onlinelibrary.wiley.com/doi/abs/10.1111/camh.12330 This is unsurprising. It is likely that the original problem remains unresolved, if a gender distressed child is only offered one of many solutions.
Furthermore, it is questionable whether social transition itself is actually as reversible as it may seem. For a child that has been conditioned to believe they are the opposite sex, the pressure becomes greater for them to continue to present as such. One study observed that once a child has been affirmed in their new gender, it is very difficult for them to desist, because they have already required those around them to affirm their transition.224T. Steensma, R.Biemond, F.de Boer et al, Desisting and persisting gender dysphoria after childhood: A qualitative follow-up study, ld Psychol Psychiatry. 2011 Oct;16(4):499-516. https://pubmed.ncbi.nlm.nih.gov/21216800/ Regardless, social transition does very often mark the beginning of a pathway that leads to irreversible and physical medical intervention. As outlined in a previous chapter, almost 100 per cent of children who take puberty blockers proceed to take cross-sex hormones.225https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0243894 The Interim Cass Report notes that stage two and three of the GIDS pathway are therefore effectively different stages of the same pathway:
The most difficult question is whether puberty blockers do indeed provide valuable time for children and young people to consider their options, or whether they effectively ‘lock in’ children and young people to a treatment pathway which culminates in progression to feminising/ masculinising hormones by impeding the usual process of sexual orientation and gender identity development.226The Cass Review, pg.38.
Uncritical affirmation of a child’s gender identity therefore comes with tangible risks. Firstly, considering the strong correlation between gender distress and other factors explored in chapter six, affirmation as a solution will likely fail, because in most cases a child’s distress is a transient symptom of another cause. Consequently, there will be a large number of children who transition in an attempt to cure their distress, only to continue to suffer with it. Secondly, the irreversible medical nature of the affirmative pathway is irreconcilable with the fact that children are much more likely to inhabit transient identities than adults. As the Interim Report notes: ‘some children and young people will remain fluid in their gender identity up to early to mid-20s.’227The Cass Review, pg.36. As aforementioned, a very small number of children may proceed to inhabit stable transgender identities as adults. However, given the lack of data on the current phenomenon, it is very difficult for clinicians to differentiate this cohort. It is particularly impossible for schools, because they are not clinical settings.
In light of this, the current practice of gender affirmation within schools highlights substantial safeguarding breaches.
8.2 Multi-agency working is being compromised
Since so many schools are facilitating social transition outside of the clinical context, it is clear that the safeguarding norm of multi-agency working is being eroded. Schools are required to co-operate with local authority partners where necessary. According to polling conducted in April 2022 by Human Rights organisation Sex Matters, 79 per cent of teachers said their school had a pupil identifying as transgender or non-binary.228Sex Matters, Most secondary schools now have trans-identified pupils: Sex Matters’ new survey, 11 April 2022. https://sex-matters.org/posts/updates/school-survey/ Yet between 2021-22 there were 3585 referrals to GIDS.229This does not to negate the fact that this number is large considering previous years. Source: Gender Identity Development Service, Number of referrals to GIDS. The inference is that the majority of children identifying as transgender or experiencing gender distress are not under clinical care. The implication of this for schools is concerning, because schools should not be facilitating medical treatments. Given the procedures schools must enact simply to be able to give paracetamol to students on their premises, the fact that so many schools are operating policies of gender self-identification is surprising.
As stated earlier, multi-agency working protects both students and staff, because the principle recognises that schools will not always be best placed to resolve a safeguarding concern when it is raised. When a school enacts a policy of self-identification, it is mistakenly allowing for a medical treatment to take place without the consent of a medical professional. It is clear that many schools are cultivating an environment in which every member of staff and pupil is expected to partake in a social experiment – in the absence of consensus or expertise from multi-agency partners or parents.
8.3 Information sharing is not taking place
Our research highlights that a number of schools that are not automatically involving their DSL when a child discloses feelings of gender distress. The affirmative response to a child’s gender distress departs from every other professional response in a mental health context, where as soon as a child disclosed a mental health or safeguarding concern, the DSL would be informed. If a child disclosed to a teacher or professional that they were dating or flirting with an adult, that professional would not accept at face value that the child’s feelings of certainty or emotional understanding about that situation offset the safeguarding concern. Similarly, if a child disclosed that they were experiencing some form of restrictive eating, that child would not be affirmed in their desire not to eat. When a child expresses feelings of mental distress about their sexed body, this concern should be escalated to the DSL. There is no reason why the gravity and attention schools generally accord to other mental health conditions or safeguarding issues should not apply to gender distress. An affirmative approach is also incompatible with the concept of professional curiosity, which seeks to gain a holistic understanding of a child’s life before making assumptions about what is in the best interest for that child’s future.
A further insight revealed by our FOI research is that a small number of schools are choosing to inform ‘LGBT staff leads’ or practitioners, rather than their school’s DSL, when a child discloses gender distress. Statutory guidance is clear that the school’s DSL is responsible for all safeguarding issues. These posts in schools are not regulated, nor are the post holders necessarily trained, to deal with safeguarding issues. As stated earlier, schools engaging with external agencies must ensure the agency adheres to the school’s safeguarding policy. Bringing in an post holder such as an LGBT practitioner from an external agency to deal with an internal safeguarding issue is not appropriate – this should fall under the remit of the DSL. As explored above, some schools are even stating that children have confidentiality rights, which is untrue. Schools should not be keeping secrets – confidentiality should never be promised to a child on any matter.
8.4 The responsibilities of parents are being neglected
The undermining of parental responsibility with regard to their child’s welfare is prevalent. Returning to the comparison with other mental health conditions, a teacher or school would be expected to inform a parent immediately if their child was experiencing suicidal ideation. Schools failing to inform parents of their child’s mental health issues are not recognising that a parent’s report is a standard method for assessing a child’s mental health within the NHS.230NHS, Advice for parents: Find advice and support for parents who have children or teenagers with menta health problems. https://www.nhs.uk/mental-health/children-and-young-adults/advice-for-parents/
‘Unsupportive parents’ was a phrase used by many schools to justify why they would not inform a parent of their child’s gender distress. Affirmative practice appears to have distorted the concept of parental support. The reality is that children and their parents will not always agree, and the fact that children may fail to appreciate the boundaries set to them by their parents is very normal. Parents who do not consent to unlicensed medical intervention on their child at school are not unsupportive, and certainly do not present as an automatic safeguarding risk. The law and the safeguarding principles based upon it is very clear: ‘unless the contrary is shown’ parents should always be involved with regard to a child’s welfare.231Education Act 1996, Part I, Chapter I, Education in accordance with parental wishes. https://www.legislation.gov.uk/ukpga/1996/56/part/I/chapter/I/crossheading/education-in-accordance-with-parental-wishes The fact that parents may not be supportive of their child’s wish to change gender should not prevent a school informing them if a child has disclosed this information.
A school’s refusal to inform a parent if their child expresses feelings of gender distress also breaches the importance of information sharing. Similarly to how the expression of other mental health conditions can be symptomatic of abuse, there is a strong correlation between children who experience abuse or adverse childhood experiences (ACE) and reports of gender distress.232M.Firth, Childhood abuse and depressive vulnerability in clients with gender dysphoria, Counselling and Psychotherapy Research Volume 14, Issue 4. https://www.tandfonline.com/doi/abs/10.1080/14733145.2013.845236 Where a parent is not identified already as the abuser/safeguarding risk, the school’s default position should be to inform parents of their child’s gender distress. Multiple schools expressed the sentiment that a child would be encouraged to inform their parents of their new gender ‘when they felt ready’ or ‘in their own time’. This is a clear breach of safeguarding.
Schools that change their information management systems to reflect a child’s self-identified gender, rather than their biological sex breach The Education (Pupil Registration) (England) Regulations 2006, which requires schools to register a number of ‘particulars’ in respect to every pupil, including their name and sex.233The Education (Pupil Registration) (England) Regulations 2006, UK Statutory Instruments, 2006 No. 1751, Regulation 5. https://www.legislation.gov.uk/uksi/2006/1751/regulation/5/made This is a statutory duty to record a child’s sex, regardless of how that child self-identifies at school. Similarly, a school may record an additional name that a child wishes to be known by, but their legal name must be recorded. A child cannot change their legal name by deed poll without parental consent.
8.5 Impact on other children
There is no reason why gender-distressed children should be excluded from safeguarding practice, particularly given the additional safeguarding vulnerabilities often experienced by this cohort. However, the impact of gender affirmative care on a gender-distressed child’s peers is also often overlooked. The intervention of social transition requires the communal participation of everyone in a school, including children and staff. Given the active nature of social transition, schools must consider how implementing gender affirmative polices impact other children. In expecting all children to endorse a socially transitioned child’s new identity, a school is unwittingly compelling them to act as non-consenting partakers in delivering a course of treatment – as a condition of receiving their own education. The number of schools operating policies requiring all children to endorse a peer’s new identity are failing to adhere to safeguarding duties to comply with the law, notably the Human Rights Act 1998 and the Equality Act 2010.
Under the Equality Act, all children must be treated fairly and live free from discrimination. Sex is a protected characteristic, and a child who has changed their gender still requires protection on the basis of their legal sex. For example, a male child who has transitioned to become the female gender is still biologically and legally a male, because children are not currently able to change their legal sex. The EA does not require anyone, including children, to treat another child as if they were a member of the opposite sex.
A further consideration is the protections accorded by the Human Rights Act 1998, which protects the right to freedom of expression: ‘This right shall include freedom to hold opinions and to receive and impart information and ideas without interference by public authority and regardless of frontiers.’234Human Rights Act 1998, Schedule I, Part I, Article 10. https://www.legislation.gov.uk/ukpga/1998/42/schedule/1/part/I/chapter/9 It will likely be the case that many children wish to endorse their peer’s new identity, but this should be the choice of individual children, rather than the school’s policy. Compelled speech is concerning – a child should not be expected to say or believe that a girl is a boy or vice versa, nor should they be expected to state their own pronouns. As aforementioned, gender critical and religious beliefs are protected under the Equality Act 2010. Children have the right to hold these beliefs without infringement. Only a very small number of schools stated that they would not require other pupils to affirm a socially transitioned child. Only one school stated specifically: ‘No, I am sure you are aware that this could be seen as contravening their right to freedom of speech.’
A final consideration is the legal protections under the Human Rights Act 1998 accorded to teachers. Like their students, teachers also have the right to freedom of expression. Gender critical beliefs are protected under the law. This has important implications for employers – including those who employ teachers. Teachers cannot be discriminated against for holding gender critical beliefs and refusing to affirm a child’s gender identity. In 2019, researcher Maya Forstater’s contract was not renewed by her employer, the Centre for Global Development Europe, on the basis that she held gender critical beliefs. Forstater challenged this decision at the Central London Employment Tribunal, which ruled that her employer’s decision was correct.235Forstater v CGD Europe & Anor (Religion or Belief Discrimination, Sex Discrimination l) [2019] UKET 2200909/2019 (18 December 2019). https://www.bailii.org/uk/cases/UKET/2019/2200909_2019.html Forstater appealed the judgment, heard by the Employment Appeal Tribunal in 2021.236Forstater v CGD Europe & Ors (RELIGION OR BELIEF DISCRIMINATION) [2021] UKEAT 0105_20_1006 (10 June 2021). https://www.bailii.org/uk/cases/UKEAT/2021/0105_20_1006.html The judgement found that Forstater’s gender critical beliefs were indeed protected under Section 10 of the Equality Act 2010, meeting the requirement that they were ‘worthy of respect in a democratic society.’237Ibid.
8.6 Sexual boundaries are being compromised
A further safeguarding consideration regarding current practice is the importance of sexual boundaries in providing education. Sex segregation is an important safeguard for preventing harm. The fact that sexual boundaries are being compromised affects all children within school. Again, the EA is very clear in all instances of sex-segregation. Regardless of a child’s chosen gender, they are protected under the law on the basis of their biological sex. As such, both socially transitioned children and their peers should be segregated where appropriate on the basis of their sex, not their chosen gender.
Under the Equality Act, some forms of discrimination – including sex-based discrimination – are legal if the intervention can be justified ‘as a proportionate means of achieving a legitimate aim.’238Equality Act 2010, Part 2, Chapter 2, Discrimination. https://www.legislation.gov.uk/ukpga/2010/15/part/2/chapter/2/crossheading/discrimination While the Equality Act allows for schools to treat the sexes differently in certain circumstances, with regard to toilets and changing facilities, The School Premises (England) Regulations 2012 explicitly states:
‘Toilet and washing facilities
4.—(1) Subject to paragraph (3), suitable toilet and washing facilities must be provided for the sole use of pupils.
(2) Separate toilet facilities for boys and girls aged 8 years or over must be provided except where the toilet facility is provided in a room that can be secured from the inside and that is intended for use by one pupil at a time.
(3) Where separate facilities are provided under paragraph (1) for pupils who are disabled, they may also be used by other pupils, teachers and others employed at the school, and visitors, whether or not they are disabled.
(4) Suitable changing accommodation and showers must be provided for pupils aged 11 years or over at the start of the school year who receive physical education.’239The School Premises (England) Regulations 2012, UK Statutory Instruments, 2012 No. 1943, Regulation 4.https://www.legislation.gov.uk/uksi/2012/1943/regulation/4/made
Some schools have made all their facilities unisex in an attempt to accommodate gender-distressed children who do not feel comfortable using facilities of their sex. While it is technically permissible for schools to provide unisex toilets ‘where the toilet facility is provided in a room that can be secured from the inside and that is intended for use by one pupil at a time’, the legislation does not elucidate on what constitutes a room.240Ibid. Resultantly, schools risk breaching the law if they have made all previously sex-separated toilets unisex without fulfilling this requirement.
On a broader point – regardless of the minutiae of the law – schools that do allow children to self-identify in facilities clearly labelled for the opposite sex is inappropriate. There are a number of reasons why children and young people would feel uncomfortable with a member of the opposite sex using their single-sex facility. Adolescence is a vulnerable time, with children experiencing an array of physical and mental changes. What is more, an Ofsted review of sexual abuse in schools and colleges published in 2021 found that sexual harassment is prevalent and rising in schools, and is more prevalent by boys on girls.241Ofsted, Review of sexual abuse in schools and colleges, 10 June 2021. https://www.gov.uk/government/publications/review-of-sexual-abuse-in-schools-and-colleges/review-of-sexual-abuse-in-schools-and-colleges A school that allows gender self-identification risk compromising other students’ rights to safety, privacy and dignity.
The DfE’s 2018 non-statutory guidance Gender separation in mixed schools guidance provides clarity. Aimed at helping schools understand how they should enact sex-separation, the guidance re-iterates the legal requirements on schools to provide separate facilities:
‘It is permissible for toilet and boarding accommodation facilities to be separate as they are captured under existing statutory exceptions. Separate toilet and washing facilities must be provided for boys and girls aged 8 years and over pursuant to Regulation 4 of the School Premises (England) Regulations 2012, which falls within the exemption provided for in Schedule 22 of the Equality Act 2010.’242Department for Education, Gender separation in mixed schools, June 2018, pg.6. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/719398/Gender-separation-guidance.pdf
On the issue of sport, Section 158 of the Equality Act covers the concept of positive action. Positive action refers to legal exceptions allowed under the Act which enable people who share a protected characteristic to be segregated on the basis of that characteristic in order to overcome disadvantage.243Equality Act 2010, Part 11, Chapter 2, Section 159. https://www.legislation.gov.uk/ukpga/2010/15/section/159 Within the context of schools, pupils can be separated if there is a) disadvantage connected to their sex, b) needs are different based on sex, and c) participation in a certain activity by that sex is very low. For example, Gender separation states that it would be appropriate to teach certain elements of RSHE to single sex classes because there are different needs in this context. Similarly, the guidance gives the example of where uptake by girls is very low in Science, Technology, Engineering and Maths (STEM) subjects. Positive action here would denote measures taken to encourage girls to pursue this (and in relevant subjects, vice versa).244Department for Education, Gender separation in mixed schools: Non-statutory guidance, June 2018, pg.5. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/719398/Gender-separation-guidance.pdf
Sport is arguably the most obvious example of where single-sex exceptions are necessary in order to uphold safeguarding principles. Section 195 of the Equality Act permits single-sex sports on the basis of them being a ‘gender affected activity’ which:
‘is a sport, game or other activity of a competitive nature in circumstances in which the physical strength, stamina or physique of average persons of one sex would put them at a disadvantage compared to average persons of the other sex as competitors in events involving the activity.’245Equality Act 2010, Part 14, Section 195. https://www.legislation.gov.uk/ukpga/2010/15/section/195
In order to account for the physical differences associated with biological sex within competitive games or sports, the Equality Act allows for sex segregation. Furthermore, Sport England (the non-departmental public body under the Department for Digital Culture, Media and Sport) refers to safeguarding in sport as ‘the process of protecting children and adults from harm by providing a safe space in which to play sport and be active.’246Sport England, Safeguarding. https://www.sportengland.org/guidance-and-support/safeguarding The National Society for the Prevention of Cruelty to Children (NSPCC) and Sport England outline ten Standards for safeguarding and protecting children in sport.247NSPCC, Child Protection in Sport Unit, Standards for safeguarding and protecting children in sport, last updated: 7 September 2018. https://thecpsu.org.uk/media/445556/web_cpsustandards.pdf Notably, ‘Standard 5: Equity’ states: ‘Measures to ensure that the needs of all children and young people to be protected from abuse are addressed’ is necessary to ensure adequate safeguarding.248Ibid.
Single-sex sports is not just about fairness, but privacy and dignity too. It is well-known that adolescence is a time when young people are particularly self-conscious around the opposite sex. Furthermore, girls’ participation in sport drops off significantly during adolescence. In 2022, charity Women in Sport conducted a survey of over 4000 teenage girls and boys, finding that more than one million girls (43 per cent) disengaged with sport at secondary school. Reasons for this included: a fear of feeling judged by others, lack of confidence, pressures of schoolwork and not feeling safe outside.249Women in Sport, More Than 1 Million Teenage Girls Fall ‘Out Of Love’ With Sport, March 2022. https://womeninsport.org/press-release/more-than-1-million-teenage-girls-fall-out-of-love-with-sport/ Single-sex sports protect the privacy, dignity and fairness of both sexes.
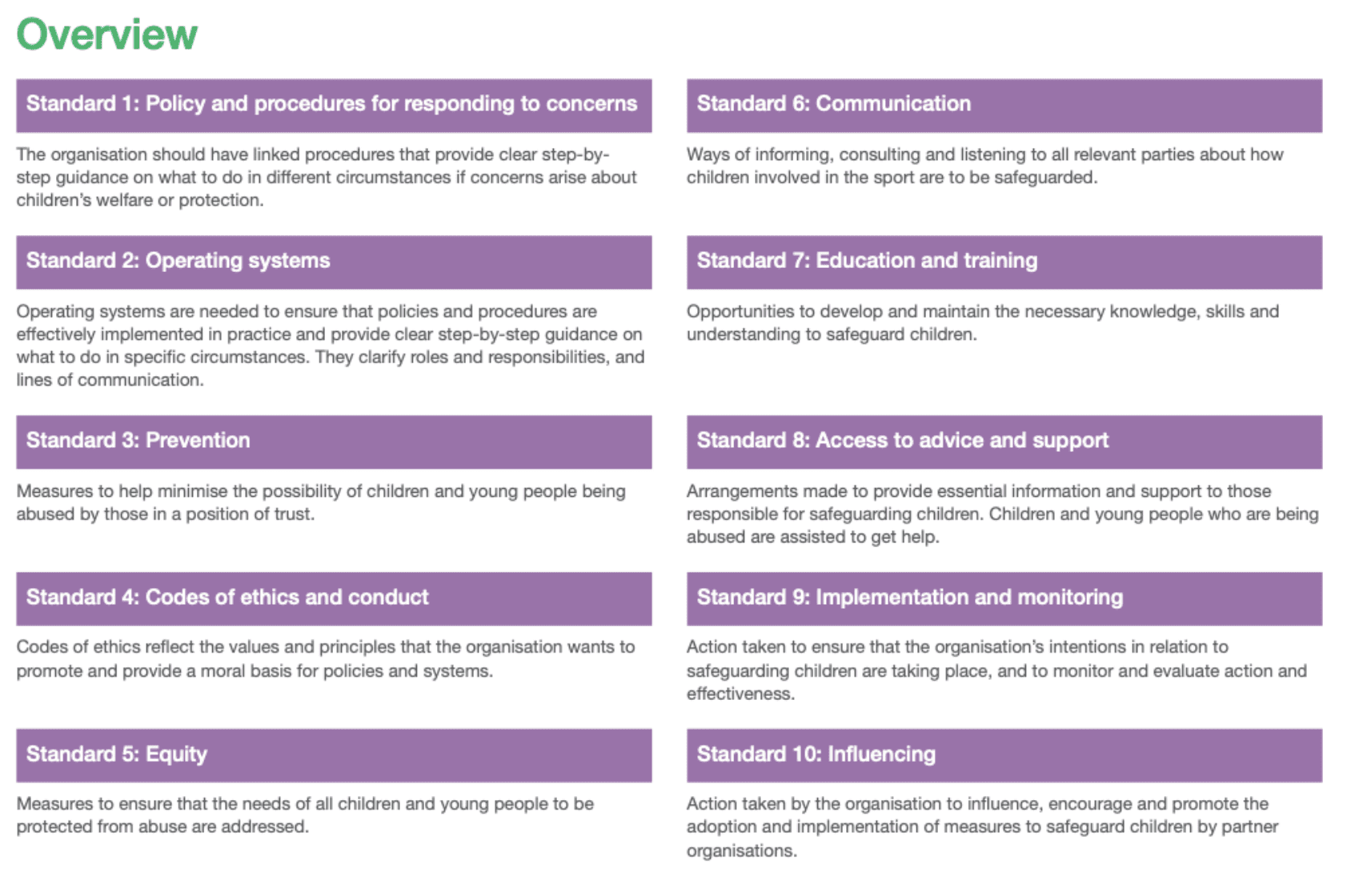
The ten safeguarding standards for children in sport set by Sport England and NSPCC.250NSPCC, Child Protection in Sport Unit, Standards for safeguarding and protecting children in sport.
A number of schools responded to our FOI question stating that all of their sports are mixed-sex, thus mitigating the need to decide whether a socially transitioned child can participate in opposite sex sports. There will be occasions where mixed-sex sports are appropriate, for example in the case of special schools or in certain activities. However, where schools set mixed-sex sports as a general rule, this is problematic – for the same reasons explained above. Guidance and the law is clear that children should be separated by sex for sports for reasons of safety and fairness. Denying the reality of biological sex does not remove sexism in sport, nor does it remove the physical risks involved with mixed-sex sports.
Next chapter9. How well is teaching on sex and gender abiding by government guidelines?
As outlined earlier, schools are expected to teach LGBT issues with political impartiality and in line with safeguarding expectations. Our research suggests many schools are departing significantly from these criteria.
Despite a number of schools referencing the importance of their pupils understanding the legal implications of Equality Act 2010 for different groups, there appears to be a much greater emphasis on teaching the characteristic of gender reassignment over sex. As results show, a surprising number of schools are teaching that ‘a person who self-identifies as a man or a woman should be treated as a man or woman in all circumstances, even if this does not match their biological sex’. This is a clear misunderstanding of the Equality Act 2010, which gives exceptions where discrimination on the basis of sex is allowed for.254Equality Act 2010, Explanatory Notes, Commentary on Sections, Part 16, Schedule 3, Part 7, Separate and single sex services. https://www.legislation.gov.uk/ukpga/2010/15/notes/division/3/16/20/7 It is important for students to be educated accurately on the sex-based rights accorded to them by the law, particularly for women and girls.
As part of the curriculum, it is clear that many schools are teaching gender identity beliefs as if they are facts. When teaching about the Equality Act, schools firstly should be presenting gender identity beliefs as beliefs, not facts. The government’s RSHE guidance is open to misinterpretation in this regard. While later guidance gives helpful clarification with regard to gender stereotypes and gender identity, the statutory guidance states: ‘Pupils should be taught the facts and the law about sex, sexuality, sexual health and gender identity in an age-appropriate and inclusive way.’255Relationships Education, Relationships and Sex Education (RSE) and Health Education, pg.26. Emphasis added. In this way the guidance fails to elucidate that gender identity beliefs are beliefs not facts. Secondly, the fact that the EA protects gender critical beliefs and religious beliefs should also be included as part of this discussion – not as something that is separate to equality or in some way in conflict with it. In the same way that discussions about religious beliefs should not exclude religious people, discussions about gender critical beliefs should not exclude those who hold them.
The conflation of sex and gender in RSHE resources is a common theme. Resources show that teaching on the reality and immutability of biological sex is being diminished. A logic which espouses that a person’s innate and ineffable feelings are more determinative of their identity than their chromosomal DNA – is frequently finding its way into the curriculum. This is demonstrated by the fact that so many schools are teaching ‘that some people or children may be ‘born in the wrong body’”. In response to this question, only one school explicitly referenced the basis of this statement as a belief: “No – this would be a political statement/bias, we would provide facts not opinion.”
Also concerning is the fact that many of the cultural and social attributes associated with genders are based on regressive stereotypes. As government guidelines make clear, teaching that encourages children to define themselves based on these stereotypes is inappropriate: ‘materials which suggest that non-conformity to gender stereotypes should be seen as synonymous with having a different gender identity should not be used.’256Gov.UK, Plan your relationships, sex and health curriculum. There is no circumstance in which a child should be encouraged to believe they have been born in the wrong body simply because they do not conform to the gender stereotypes associated with their biological sex.
The government guidance on working with external agencies is very clear – organisations which promote gender stereotypes or suggest that gender non-conformity means a child may in fact be a different sex are not appropriate. All external agencies must also understand the school’s safeguarding protocols and be aligned with them. The next chapter will explore how many of the external agencies used by schools for RSHE operate under the guise of anti-bullying, but are in fact promoting a partisan and political belief: that gender is more determinative of identity than biological sex. These organisations often promote a very simplified version of transition, which obviate the mental and physical health risks involved in affirmation. In order to understand why so many schools are departing from guidance and teaching philosophical beliefs as facts, the influence of lobbying groups on the wider education system requires explanation.
Next chapter10. How did we get here?
What led the UK’s education system to allow safeguarding principles and appropriate RSHE teaching to be so obviously compromised? This chapter will consider why the affirmative approach towards children with gender distress is so prevalent, despite departing from every other approach in a mental health context. It will also track how gender identity beliefs became crystalised as fact within the classroom.
The wider climate within the government regarding sex and gender is important. The fact that transgender activism only relatively recently became associated with wider Lesbian, Gay and Bisexual (LGB) activism is an important distinction in understanding how beliefs about gender identity came to be so embedded. The LGBT charity Stonewall played a significant and historic role in making this distinction.
Stonewall – instrumental in the struggle against homophobia
Stonewall was formed in 1989 in response to Section 28 of the Local Government Act, which prohibited the promotion of homosexuality across local authorities.257Stonewall, Stonewall’s history. https://www.stonewall.org.uk/stonewalls-history The organisation was instrumental in repealing Section 28, and by the late 1990s, Stonewall had become critical in successfully campaigning against homophobia.
In 2001, Stonewall created the Diversity Champions programme, a workplace equality scheme which employers can join to measure their progress on LGB (and now, TQ+) inclusion in the workplace. At a time when corporate social responsibility was becoming important for large businesses, Stonewall began working with a range of companies. The scheme grew, and in 2008 alone, businesses such as John Lewis, Aviva and IBM paid Stonewall for services, as well banks Barclays, Credit Suisse and Lloyds.258Stonewall, Full accounts made up to 30 September 2008. Link.
Stonewall also focused on education. In 2005, the charity launched its Workplace Equality Index (WEI) (formally known as the Corporate Equality Index). The WEI ranks employers based on their LGB (and now, TQ+) inclusion in the workplace.259Stonewall, UK Workplace Equality Index. https://www.stonewall.org.uk/creating-inclusive-workplaces/workplace-equality-indices/uk-workplace-equality-index Winners include MI5,260MI5, MI5 names employer of the year by Stonewall, 19 January 2016. https://www.mi5.gov.uk/fr/news/mi5-named-employer-of-the-year-by-stonewall Staffordshire Police261Stonewall, Workplace Equality Index 2007: The Top 100 Employers For Gay People In Britain. http://image.guardian.co.uk/sys-files/Society/documents/2007/01/09/gayfriendlyemployers.pdf and the Home Office.262Gov.UK, Stonewall announces the Home Office as top public sector employer, 11 January 2012. https://www.gov.uk/government/news/stonewall-announces-the-home-office-as-top-public-sector-employer Stonewall subsequently launched its School and & College Champion Awards, in which schools can benchmark themselves on their LGB (now TQ+) inclusion, by reaching certain criteria in order to achieve Gold, Silver or Bronze awards.263Stonewall, Stonewall School & College Champion Membership. https://www.stonewall.org.uk/stonewall-school-college-champion-membership
Stonewall also gave out annual awards to people or organisations who ‘had a positive or negative impact on the lives of British lesbian, gay and bisexual people’ (now also transgender people).264Stonewall, Our Award Winners 2022. https://www.stonewall.org.uk/our-work/campaigns/our-award-winners-2022 Between 2006 and 2015, there was a politician of the year category. Notable winners included John Bercow,265Stonewall, John Bercow. https://www.stonewall.org.uk/john-bercow Chris Bryant266LGBT History Archive, Stonewall Awards 2011. https://lgbthistoryuk.org/wiki/Stonewall_Awards_2011 and Ruth Davidson.267Conservative Home, Scottish Tory leader Ruth Davidson jeered at Stonewall awards ceremony after she questions “Bigot of the Year” category, 2 November 2012. https://conservativehome.com/2012/11/02/scottish-tory-leader-ruthdavidsonmsp-is-jeered-at-stonewall-awards-ceremony-after-she-questions-bigo/ The award was reputable, as evidenced by this tweet from Lynne Featherstone, who had just been appointed Minister of State for Crime Prevention as part of the Coalition Government.268Twitter, Lynne Featherstone, 8 November 2014: 6:00PM. https://twitter.com/lfeatherstone/status/531144296645537793

Between the years 2003 and 2014, the following government departments awarded grants to Stonewall:
- HM Prison Service
- Welsh Assembly Government
- Department of Trade and Industry
- Equalities and Human Rights Commission
- Department for health
- Home Office
- Scottish Government
- Greater London authority
- Foreign Commonwealth Office
In 2005, the charity launched an ‘Education for All’ (EfA) programme, in partnership with the NSPCC and Barnardo’s, to help fight homophobic bullying in schools.269Stonewall, 2005: Stonewall’s Education for All campaign is launched: teaching love and talking bullying. https://www.stonewall.org.uk/our-work/campaigns/2005-stonewall%E2%80%99s-education-all-campaign-launched-teaching-love-and-tackling Politicians often spoke at the EfA annual conference, demonstrating cross-party support:
- In 2012, Stephen Twigg, as Shadow Secretary of State for Education.270Twitter, Stephen Twigg, 5 July 2012: 9:11AM. https://twitter.com/StephenTwigg/status/220791976226852864
- In 2014, Charlie Taylor, as Chief Executive of National College of Teaching and Leadership.271Association for Physical Education, Stonewall – Education for All Conference 2014. https://www.afpe.org.uk/physical-education/event/stonewall-education-for-all-conference-2014-2/
- In 2015, Nikki Morgan, as Education Secretary.272Gov.UK, Speech: Nicky Morgan speaks about tackling LGBT bullying, 10 July 2015. https://www.gov.uk/government/speeches/nicky-morgan-speaks-about-tackling-lgbt-bullying
- In 2016, Yvette Cooper as Shadow Home Secretary.273Stonewall, Yvette Cooper addresses delegates: Stonewall Education for All Conference. https://www.stonewall.org.uk/about-us/news/yvette-cooper-addresses-delegates-stonewall-education-all-conference
In 2013, in a parliamentary debate on the national curriculum, then Secretary of State for Education Michael Gove said:
“The hon. Lady is a passionate campaigner on ways we can better protect our children, and there are a number of things we can do. As she may know, I had the opportunity to talk to a group of outstanding young people last week at the Stonewall conference on fighting prejudice in education and empowering young people. They made some important points about the best of personal, social, health and economic education, and we must learn from the best schools and ensure that others follow their lead.”274Hansard, National Curriculum, Volume 566: debated on Monday 8 July 2013. https://hansard.parliament.uk/Commons/2013-07-08/debates/13070810000004/NationalCurriculum?highlight=stonewall#contribution-13070810000319 (emphasis added)
Stonewall quickly became the authoritative voice on LGB education, launching a range of programmes including educational resources, an Educational Equality Index (EEI) mirrored on the WEI, as well as a Children’s and Young People’s Service Champions programme, aimed at local authorities, youth organisations and multi-academy trusts.275Stonewall, Children’s and Young People’s Services Champions programme. https://www.stonewall.org.uk/children-and-young-peoples-services-champions-programme
It is difficult to find a definitive list of all the councils and schools that were working with Stonewall by 2015. In the Trustee report for 2014-2015, it is clear their influence in the education system was vast. During this year, Stonewall had:
- trained nearly 700 teachers on homophobic, biphobic and transphobic (HBT) bullying
- sent resources to 46,000 individuals and organisations
- trained more than 60 local organisations to deliver Stonewall programmes to local schools (est. reach 12000 pupils by 2016)
- reached 5000 pupils through their School Role Models programme.276Stonewall, Full accounts made up to 30 September 2015. Link.
In 2015, 47 local authorities had entered Stonewall’s Education Equality Index.277UNESCO, Stonewall education equality index 2015. https://healtheducationresources.unesco.org/library/documents/stonewall-education-equality-index-2015-celebrating-difference-and-preventing-and?language=fr
With the support of big business, cross-party political endorsement, local authorities and government funding, Stonewall had become the authoritative voice on LGB education within schools.
The absence of the T from Stonewall’s LGB mission becomes noticeable
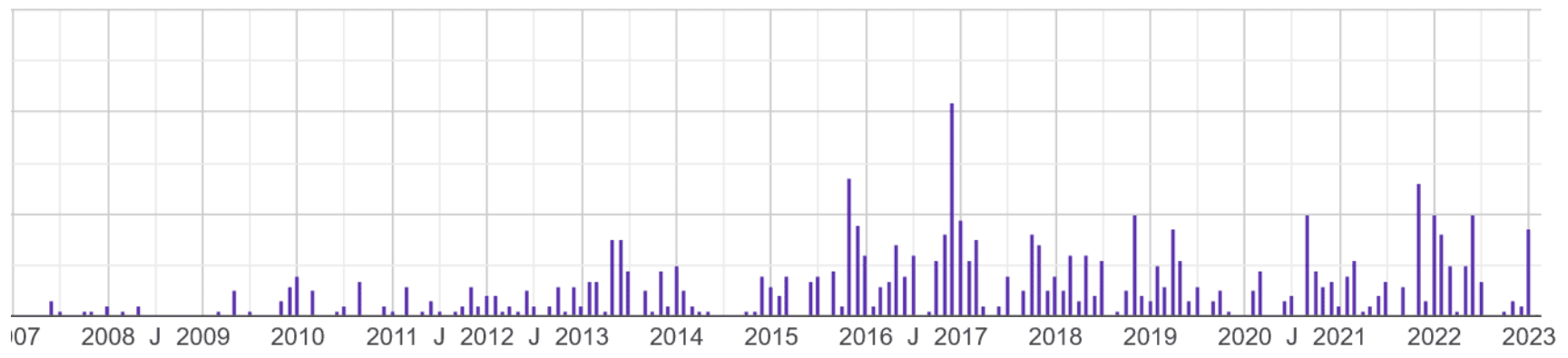
Searching for the use of the word ‘transgender’ in parliamentary debates demonstrates that the trans issue was rarely on the political agenda.278Hansard, Find in Hansard ‘transgender’. https://hansard.parliament.uk/search?startDate=2007-03-20&endDate=2023-03-23&searchTerm=transgender&partial=False
With its focus on LGB people, Stonewall appeared to be indifferent to the transgender mission. It was even criticised by transgender campaigning groups. In 2008, lesbian journalist Julie Bindel was awarded Stonewall’s journalist of the year. This resulted in an 150-person protest outside of the award ceremony, as Bindel was seen as hostile to the transgender movement.279Pink News, Celebs split over trans protest at Stonewall Awards, 8 November 2008. https://www.thepinknews.com/2008/11/07/celebs-split-over-trans-protests-at-stonewall-awards/ In 2010 Pink News reported that Stonewall had been criticised again over one of five nominees for the gay charity’s annual Journalist of the Year award.280Pink News, Trans group angry at Stonewall’s nomination of journalist it criticised, 14 October 2010. https://www.thepinknews.com/2010/10/14/trans-group-angry-at-stonewall-nomination-of-transphobic-journalist/
In 2010, a Guardian article accused Stonewall of excluding transgender people, with transgender journalist and academic Dr Natacha Kennedy/Mark Hellen writing: ‘Despite running its “diversity champions” programme, we are clearly not the sort of diversity Stonewall wants.’281N.Kennedy, Stonewall is holding back transgender equality, The Guardian, 20 October 2010. https://www.theguardian.com/commentisfree/2010/oct/20/stonewall-holding-back-transgender-equality

In 2014, a member of Gendered Alliance, a charity which seeks to increase understanding of gender diversity and improve transgender people’s lives, criticised Stonewall in an interview entitled ‘Does Stonewall actively ignore the ‘T’ in LGB?’282Youtube, Does Stonewall actively ignore the ‘T’ in LGBT?, 5 September 2014. https://www.youtube.com/watch?v=imNEgzY2EBc
As late as July 2014, Stonewall’s website logo made no reference to transgender people.283Web Archive, Stonewall, 4 July 2014. https://web.archive.org/web/20140704083551/http://www.stonewall.org.uk/

Stonewall becomes an LGBT charity
In August 2014, Ruth Hunt was announced as the new CEO, having worked with Stonewall since 2005.284Twitter, Stonewall, 5 August 2014: 9:30PM. https://twitter.com/stonewalluk/status/496755044952182785 Within three months, Stonewall had launched its first transgender campaign, which involved promoting merchandise with the logo: ‘SOME PEOPLE ARE TRANS. GET OVER IT!’285Twitter, Stonewall, 24 October 2014: 1:15PM. https://twitter.com/stonewalluk/status/525621495305732096 By December 2014, Stonewall was publishing advice for LGBT role models.286Web Archive, Stonewall, 13 December 2014. Emphasis added. web.archive.org/web/20141213061445/http://www.stonewall.org.uk/media/current_releases/10243.asp

Given Stonewall’s mission had been entirely focused on LGB people, it is possible that the decision to turn to transgender activism may have been based on the growing criticism the charity was facing for excluding the T from their LGB focus. Despite their 26-year legacy of unprecedented success in tackling homophobia and improving the lives of LGB people, in February 2015 Hunt apologised on behalf of the charity:
‘Over the last four months, I’ve spoken to hundreds of trans people who say we were wrong to maintain that distinction and we made it worse by making mistakes.
We recognise the impact of mistakes we have made in the past. We are aware that we have missed opportunities to open up this conversation far sooner. We apologise to trans people for the harm that we have caused.’287A.Gani, Stonewall to start campaigning for trans equality, The Guardian, 16 February 2015. https://www.theguardian.com/uk-news/2015/feb/16/stonewall-start-campaigning-trans-equality
In this statement, Hunt is referring to the consultation Stonewall ran in late 2014 on how the charity could become trans-inclusive. Over 700 transgender people took part, and the disclosure of their experiences formed the basis of Stonewall’s new mission. 288Stonewall, A Vision for Change. https://www.stonewall.org.uk/vision-change
In 2015, Stonewall also launched its ‘Trans Advisory Group’ to help develop their transgender strategy. Stonewall has removed this webpage, but it is available as an archive.289Web Archive, Stonewall, 24 April 2016. https://web.archive.org/web/20160424184439/https://www.stonewall.org.uk/trans-advisory-group The group consists of a range of transgender activists, including those who were running their own campaigning groups, such as Sarah Brown of TransDocFail and Tara Stone of Be: Trans Support & Development North. Helen Belcher (who has now been awarded an OBE) is listed on the page as ‘Secretary of the Parliamentary Forum on Gender Identity.’ An FOI response from 2013 disclosed that this committee held no relation to parliament.290WhatDoTheyKnow, Parliamentary Forum on Gender Identity, 18 July 2013. https://www.whatdotheyknow.com/request/parliamentary_forum_on_gender_id
| The reason for outlining how Stonewall formed its transgender mission is important. As schools, businesses and government departments were outsourcing their LGB strategy to Stonewall, with no internal expertise of its own, it appears Stonewall was outsourcing its own ‘T’ strategy to transgender activists. As the authoritative voice that had become so well-established within classrooms, HR departments and local councils across the UK, presumably it was felt there was little need to scrutinise Stonewall on the credibility of its new mission. |
Stonewall’s mission changed but it retains its influence
By 2015, Stonewall had been endorsed by thousands of schools in UK and had a close working relationship with many government departments. Having been vetted and cleared under a very different aim, there was little to stop their new agenda being adopted in their vast network of schools, academy trusts and councils – despite having undergone a fundamental change of strategy.
Stonewall was founded on the premise that homosexual people deserve to live free from discrimination and be treated as equals to heterosexual people. There is no medical intervention associated with a child that comes out as gay, lesbian, or bisexual. Nothing in this mission diminishes the reality and immutability of biological sex. Stonewall’s transgender rights movement is considerably more complex. This is because it sets out as a static and objective reality that every child has an innate sense of their gender which is by default more determinative of their identity than their sex. Given the primacy accorded to gender identity, the only viable solution when presented with a gender-distressed child is affirmation. Stonewall’s solution is presented very simply: affirmation to the point of irreversible medical intervention is necessary in order to respect the authority of a child’s gender identity – even if this treatment is not ultimately in the child’s best interests.
The conflation of their LGB mission with their new mission for transgender rights enabled Stonewall to retain their influence. In 2015, the DfE and GEO announced a joint £2mn for eight organisations with the aim of eradicating HBT bullying. Stonewall received the largest share of the fund, nearly £500,000.291Gov.UK, Press release: Awards announced from £2 million homophobic bullying fund, 24 March 2015.
https://www.gov.uk/government/news/awards-announced-from-2-million-homophobic-bullying-fund
In 2016, a further three year £4.6mn anti-bullying fund was announced, again split between the DfE and GEO. The GEO was allocated a budget of £3mn for organisations working against HBT bullying.292Gov.UK, All Different, All Equal: How we’re investing in tackling bullying in schools, 15 November 2017.
https://equalities.blog.gov.uk/2017/11/15/all-different-all-equal-how-were-investing-in-tackling-bullying-in-schools/ Stonewall, the LGBT Consortium and the Proud Trust were among the recipients.
Below is breakdown of government funding Stonewall received to deliver HBT training:
| Year | Grant | Department |
| 2015-2016 | £211,350293Stonewall, Full accounts made up to 30 September 2016. Link. |
Department for Education |
| 2016-2017 | £146,897294Stonewall, Full accounts made up to 30 September 2017. Link. |
Department for Education |
| 2017-2018 | £233,673295Stonewall, Full accounta made up to 30 September 2018. Link. |
Department for Education |
| 2018-2019 | £299,611296Stonwall, Full accounts made up to 30 September 2019. Link. |
Department for Education |
| 2019-2021 | £50,393297Stonewall, Full accounts made up to 31 March 2021. Link.Note: Stonewall changed their financial year from September to March, so accounts ran from Sept 2019-March 2021. |
Government Equalities Office |
According to an FOI response, the DfE also worked internally with Stonewall. Between 2017 and 2021, the department paid over £21,000 for various services, including annual membership to the Diversity Championship Scheme and attendance at a conference. As part of this sum, £6000 was spent on the Stonewall LGBTQ+ Allies Programme, which aims to educate workplaces on LGBTQ+ Allyship.298WhatDoTheyKnow, Information about your funding to Stonewall or any subsidiary of Stonewall, 9 November 2021. https://www.whatdotheyknow.com/request/information_about_your_funding_t#incoming-1941237 The DfE’s permanent secretary from 2016 to 2020 Jonathan Slater won Stonewall Senior Champion of the Year in 2019.299B.Smith, ‘There’s been a lot of listening’: Jonathan Slater on becoming civil service LGBTI champion, Civil Service World, 4 July 2019. https://www.civilserviceworld.com/in-depth/article/theres-been-a-lot-of-listening-jonathan-slater-on-becoming-civil-service-lgbti-champion
With vast amounts of public money behind them and the DfE itself fully subscribed, Stonewall began producing a number of school resources in which they again outsourced the ‘T’ in their mission by collaborating with transgender charity Gendered Intelligence – the same charity whose spokesperson had criticised them several years earlier. Stonewall states at the beginning of Getting Started: A toolkit for preventing and tackling homophobic, biphobic and transphobic bullying in secondary schools (2015) ‘We are hugely grateful to Gendered Intelligence for their support in making this resource trans-inclusive’.300Stonewall, Getting Started: A toolkit for preventing and tackling homophobic, biphobic and transphobic bullying in secondary schools, 2015. https://www.stonewall.org.uk/system/files/secondary_gstk_eng_singles-ap2_-_final_edited_-_march_2022.pdf

The safeguarding section within Getting Started explicitly compromises several safeguarding principles: that of information sharing and parental involvement in a child’s life.301Ibid, pg.19.
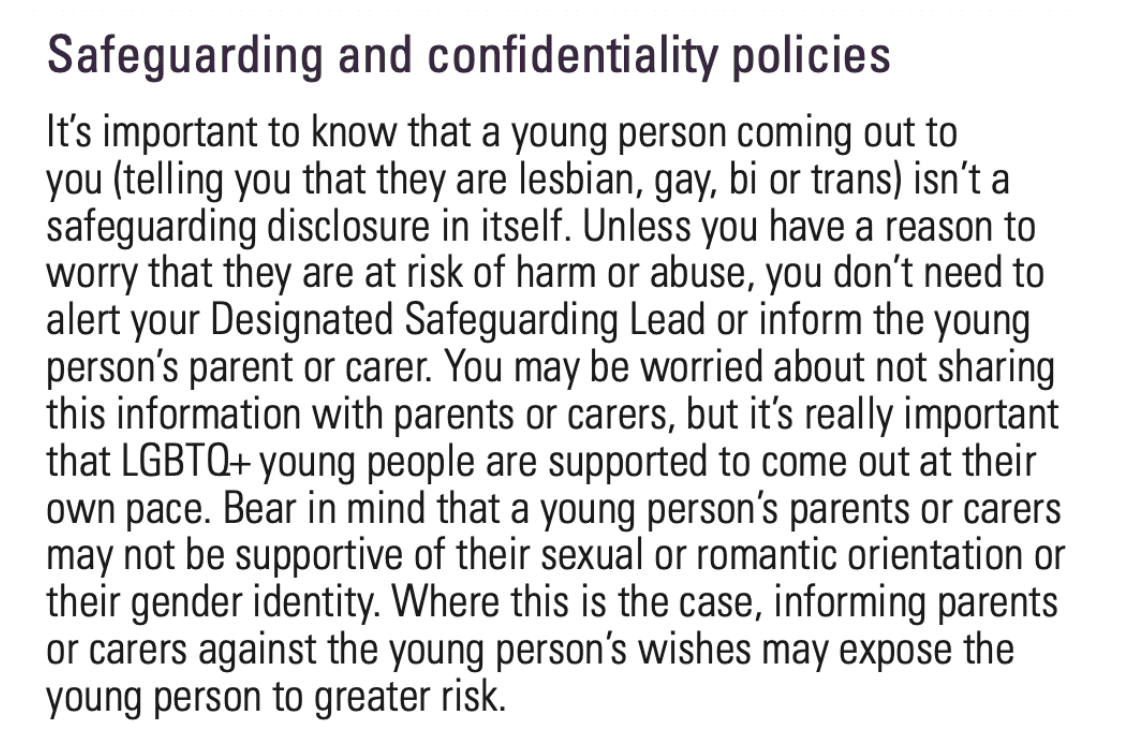
This is a clear example of how Stonewall moved away from educating schools on their legal and ethical obligations for equality, and began advising them to go beyond the law in order to embed political beliefs within their ethos. Again, Stonewall appears to conflate parents who do support affirmation as ‘unsupportive’. The presentation of parents as automatic risk is fundamentally incompatible with safeguarding principles, where a practitioner is to assume, unless the contrary is shown, that parents have responsibility for their child’s welfare. As this report has demonstrated, Stonewall’s conflation of gay rights with gender identity is problematic when viewed through the lens of safeguarding, because affirmative practice associated with gender identity beliefs is not a one-size-fits-all solution. A child that expresses gender distress is always a safeguarding matter – and therefore the school’s DSL should be informed, as well as the child’s parents.
In 2020, Stonewall published ‘An Introduction to Supporting LGBT Young People’ which encourages schools to compromise sexual boundaries by allowing children to use facilities and take part in sports that match their gender identity, rather than their sex.302 Stonewall, An Introduction to supporting LGBTQ+ children and young people: A guide for schools, colleges and settings, 2020, pg.45. page 45 https://www.stonewall.org.uk/sites/default/files/final_-_an_intro_to_supporting_lgbt_young_people_-_april2022.pdf The guidance explicitly misstates the Equality Act 2010, implying that the single-sex exceptions allowed for under the law are based on gender, not sex.303Ibid.
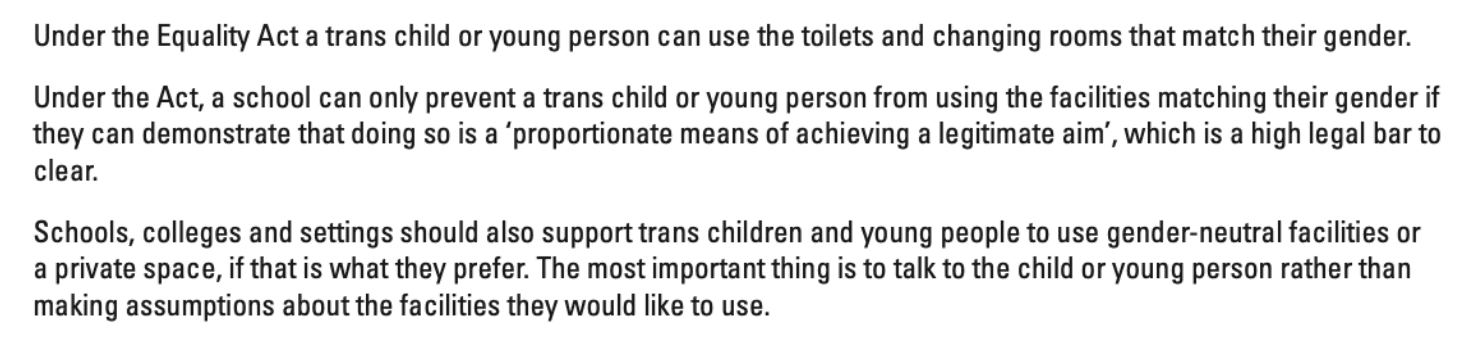
Prior to 2015, much of Stonewall’s membership offering was based on the premise that they could help schools ensure they were abiding by relevant equalities legislation, while promoting the importance of LGB education. While the influence within government remained, the mission had changed. Stonewall began lobbying for a political ideology at the highest levels of government.
A much wider web of organisations involved in providing education have engaged with Stonewall. Social enterprise Teach First co-ordinates a teacher training programme and is the largest recruiter of graduates in the UK. Since its inception in 2002, Teach First has placed nearly 12,000 teachers in low-income areas.304TeachFirst, Our impact. https://www.teachfirst.org.uk/our-impact In 2022, the charity received a gold award in Stonewall’s WEI and reached 33 in the Stonewall Top 100 Employers list.305TeachFirst, Teach First’s LGBTQ+ inclusion journey, 23 February 2022. https://www.teachfirst.org.uk/blog/lgbtq-inclusion-journey
Ofsted has also worked with Stonewall. Their LGBTQ+ staff network group Ofsted Rainbow Alliance joined Stonewall’s Diversity Champions programme in 2018.306WhatDoTheyKnow, WEI Submission Evidence, pg.12. https://www.whatdotheyknow.com/request/724316/response/1911566/attach/11/Ofsted%20WEI%20Submission%20Evidence.pdf?cookie_passthrough=1 In 2019, they entered the WEI, scoring 319th out 445 participants.307WhatDoTheyKnow, Ofsted Workplace Equality Index 2019: Feedback Report. https://www.whatdotheyknow.com/request/883093/response/2110096/attach/3/Stonewall%20WEI%202019%20CLIENT%20REPORT%20Ofsted.pdf?cookie_passthrough=1 In 2020, they scored 208th out of over 500 participants.308WhatDoTheyKnow, Ofsted: Workplace Equality Index 2020 Feedback.https://www.whatdotheyknow.com/request/724316/response/1911566/attach/8/Stonewall%20Written%20Feedback%20Report.pdf?cookie_passthrough=1
Stonewall praised Ofsted for promoting LGBT equality in the schools they inspect.309Ibid. In Section 9 of their WEI feedback report ‘Clients, customers and service users’ Stonewall said:

In 2019, Chief Inspector Amanda Spielman spoke at Stonewall’s first ever Children and Young People Conference.310Gov.UK, Amanda Spielman at Stonewall. 5 July 2019. https://www.gov.uk/government/speeches/amanda-spielman-at-stonewall In June 2022, The Telegraph reported that Ofsted had been downgraded schools’ ratings, citing ‘lack of teaching on gender identity’ as a reason.311E.Somerville, Ofsted cites lack of gender identity lessons as factor in primary school grading, The Telegraph, 18 June 2022. https://www.telegraph.co.uk/news/2022/06/18/ofsted-cites-lack-gender-identity-lessons-factor-primary-school/
Concerns about Stonewall’s agenda have been growing over the last several years. In March 2021, Ofsted confirmed they had paused their membership to Stonewall.312WhatDoTheyKnow, Information about your dealings with Stonewall. 4 February 2021.https://www.whatdotheyknow.com/request/724316/response/1744458/attach/4/210312%20Ermine%20Amies%20Stonewall%20FOI%20letter.pdf?cookie_passthrough=1 In 2022, the then Education Secretary Michelle Donelan stated that DfE’s Stonewall membership had expired. She confirmed that the department would not be renewing it.313UK Parliament, Department for Education: LGBT+ People, IUN139565, tabled on 14 March 2022. https://questions-statements.parliament.uk/written-questions/detail/2022-03-14/139565/
With Stonewall’s endorsement of gender identity beliefs fully embedded within schools, a number of other organisations with similar missions have begun working with schools, some of which received significant government funding. Similarly to Stonewall, all of these organisations work under umbrella aims of LGBT inclusion and anti-bullying. The Proud Trust, its affiliated award scheme the Rainbow Flag Award and Diversity Role Models were organisations named by some of the schools we sent FOI requests to. Below is analysis of some of their teachings.
The Proud Trust
A large number of schools we asked had worked with the Proud Trust (TPT), either directly or through downloadable resources. TPT is an external provider of RSHE resources for both primary and secondary schools. The charity describes itself as ‘a life changing charity providing education, support and advocacy for LGBT+ young people and their communities.’314The Proud Trust, About Us. https://www.theproudtrust.org/about-us/
TPT hosts LGBT+ youth groups, as well as LGBT+ awareness training, education and resources for schools. Very few of these resources are publicly available on their website. It also runs a live chat service with LGBT+ mentors and an additional mentorship scheme. It is not clear from TPT’s website how these mentors are selected, trained or vetted, as there is no policy listed online.
Like Stonewall, TPT is based on gender identity beliefs which are presented as facts. Both Safe Schools Alliance (SSA) and Transgender Trend (TT) have produced research briefings outlining the problematic nature of TPT’s resources.315Safe Schools Alliance, Parents’ guide to external PSHE/RSE providers, https://safeschoolsallianceuk.net/wp-content/uploads/2020/10/Parents-Guide-to-external-PSHE-RSE-providers.pdf, Transgender Trend, Schools Resources. https://www.transgendertrend.com/schools-resources/
Since these documents were produced, several of the links outlining previously publicly available resources have been removed from TPT’s website. One screenshot captured by SSA forms part of TPT’s Know your rights at school and college document, and states that children ‘have the right’ to use whichever toilet they feel ‘comfortable using’.316Ibid.
Further highlighted by SSA is TPT’s Sex and relationship guide for lesbian and bisexual women from 2016, which remains on their website.317The Proud Trust, It Aint What You Do, It’s The Way That You Do It: A sex and relationshops guide for lesvbian and bisexual women by the Young Women’s Health Project 2016. https://www.theproudtrust.org/wp-content/uploads/download-manager-files/digital_TPT%20sex%20rel%20guide.pdf In its glossary it offers a definition of lesbian which is completely at odds with what same-sex attraction actually is – which is attraction to the same sex, not same gender. As SSA highlights: ‘Stating that a lesbian is someone who identifies as a woman means that men can claim to be lesbians; this is homophobic and contributes to a culture in which lesbians are pressured to have sex with men.’318Safe Schools Alliance, Parents’ guide to external PSHE/RSE providers

It is clear from this small snapshot that resources from TPT fully subscribe to gender identity beliefs and present them as facts. Furthermore, part of TPT’s offering for secondary schools is the ‘The Sexuality Gender Toolkit’ aimed at pupils from age 13.319The Proud Trust, Inclusive RSE – The Sexuality Agender Toolkit. https://www.theproudtrust.org/schools-and-training/secondary-resources/inclusive-rse-the-sexuality-agender-toolkit/ Organisation Transgender Trend explains what the kit consists of.320S.Charlesworth, The Proud Trust: Nothing to be Proud of, Transgender Trend, 20 May 2020. https://www.transgendertrend.com/proud-trust-nothing-proud/ The toolkit offers several lesson plans, one of which endeavours to educate young people to communicate with their partners ‘about the kinds of sexual activities they might want to do now and in the future.’321The Proud Trust, Inclusive RSE – The Sexuality Agender Toolkit. In another lesson, pupils can play a dice game which features various genital body parts, and in partners, pupils must discuss which sexual activities might occur between those parts.
Since 2017, several Government departments including GEO, DfE, DCMS and DWP have paid TPT just over £620,000.322Charity Commission for England and Wales, The Proud Trust LTD, Acounts and annual returns. https://register-of-charities.charitycommission.gov.uk/charity-search/-/charity-details/5048520/accounts-and-annual-returns Between 2017-2019, the DfE and GEO gave almost £360,000 for ‘delivery of whole school approach to combating homophobia, biphobia and transphobia’ which included the funding of the aforementioned RFA. Between 2018-2020, the Department of Culture, Media and Sport (DCMS) paid over £100,000 ‘towards a programme of activities to benefit LGBT and pansexual women and to increase their civic engagement.’323The Proud Trust, The Proud Trust Ltd, Financial Statements for the year ended 31 March 2018. Link. This came out of the Government’s Tampon Tax Fund, the purpose of which is to donate the Value Added Tax (VAT) paid on sanitary products to projects that improve the lives of disadvantaged women and girls.324The Proud Trust, The Proud Trust Ltd, Financial Statements for the year ended 31 March 2019. Link. It is unclear why TPT received funding from this source given its purpose. The last recorded government payment was made by the DWP, for the sum of £521 in 2021.325The Proud Trust, The Proud Trust Ltd, Financial Statements for the year ended 31 March 2021. Link.
The Rainbow Flag Award
Several schools informed us that they had received The Rainbow Flag Award (RFA). The RFA grew out of a GEO funded pilot, as a ‘national quality assurance framework’ which is awarded to schools if they meet certain criteria. The RFA is a franchise offered by TPT, but which is delivered by local LGBT communities in a school’s local area. It is not clear how these external organisations are vetted or chosen to deliver the training. To achieve the award, schools must engage with a series of courses, resources and lesson plans which are delivered by network of LGBT organisations across the UK. Participation costs between £795 and £1050.326The Rainbow Flag Award, FAQ’s. https://www.rainbowflagaward.co.uk/faq/ As highlighted by Transgender Trend (TT), ‘since the pilot scheme new government guidance on outside agencies operating in schools has been published. Head teachers should also know that much of the RFA content is now in breach of the 2020 guidance on the planning of the relationships, sex and health curriculum.’327Transgender Trend, The Rainbow Flag Award, 18 July 2021. https://www.transgendertrend.com/rainbow-flag-award/

The RFA was seed-funded by The Government Equalities Office (GEO) and the Department for Education (DfE) between 2017 and 2019 as part of a £4.4million anti-bullying fund.328Gov.UK, Press release: Thousands more children to benefit from anti-bullying app, 8 September 2016.https://www.gov.uk/government/news/thousands-more-children-to-benefit-from-anti-bullying-app It began as a pilot project of The Proud Trust, an LGBT charity which provides school’s training programmes. On its website, the RFA addresses accusations that it breaches the Government’s RSE guidelines on teaching about gender stereotypes, stating ‘our work does not fall in scope of these concerns.’329The Rainbow Flag Award, FAQ’s. The RFA appears to issue awards based on its own standards, and is not monitored by any external agency or regulator.
Diversity Role Models

Diversity Role Models (DRM) is another LGBT charity that provides workshops and resources for schools. Despite offering to provide free downloadable resources, none of these are available for schools or parents to view on their website.330Safe Schools Alliance UK, ‘Love has no age’: a letter to Asda, 18 June 2020. https://safeschoolsallianceuk.net/2020/06/18/love-has-no-age-a-letter-to-asda/
In 2020, DRM partnered with supermarket Asda, which included a £100,000 donation.331https://www.asda.com/good-living/article/george-partners-with-role-models-for-pride Also included in this partnership was a LGBT home learning pack as the country was in lockdown because of Covid-19 when the partnership was announced. SSA analysed the pack, which contained a video and associated worksheet about acceptance containing the phrase ‘love has no age’.332Safe Schools Alliance UK, ‘Love has no age’: a letter to Asda. As outlined by SSA, this is a phrase commonly associated with paedophiles. SSA also notes how the pack contained a book recommendation to ‘Beyond Magenta: Transgender Teens Speak Out’, a highly controversial book in which a child aged 6 is depicted as performing a consensual oral sex act – this is obviously not possible. After SSA wrote to Asda highlighting the content of the pack, Asda apologised and removed the material.
DRM has again received significant financial support from the Government. It received over £150,000 from GEO in 2016, which was dedicated towards providing staff training on HBT bullying.333Diversity Role Models, Annual Report and Financial Statements for the year ended 31 August 2016. https://www.diversityrolemodels.org/media/1371/annual-report-and-financial-statements-2016.pdf In 2017, nearly £10,000 was given by the Home Office ‘for a project’ working with schools in London.334Diversity Role Models, Annual Report and Financial Statements for the year ended 31 August 2017. https://www.diversityrolemodels.org/media/1058/annual-report-and-financial-statements-2017.pdf Nearly £100,000 was awarded again by GEO in 2019 for a continuation of the HBT bullying training.335Diversity Role Models, Annual Report and Financial Statements for the year ended 31 August 2019. https://www.diversityrolemodels.org/media/1500/annual-report-and-financial-statements-2019.pdf A GEO press release from 2019 entitled ‘LGBT History Month: new government support for LGBT groups’ named DRM alongside Barnardos, Stonewall, the National Children’s Bureau and Equaliteach as part of a £1mn fund to tackle LGBT bullying.336Gov.UK Press release: LGBT History Month: new government support for LGBT groups, 1 February 2019. https://www.gov.uk/government/news/lgbt-history-month-new-government-support-for-lgbt-groups Most recently, a further £187,000 has been paid to DRM for new anti-bullying projects.337UK Parliament, Equality, Question for Department for Education, UIN 94270, tabled on 16 December 2021. https://questions-statements.parliament.uk/written-questions/detail/2021-12-16/94270
Next chapter11. Putting safeguarding first
This report has sought to demonstrate that gender distress in children is a complex condition that requires thoughtful decision making. School is not the setting in which these complexities can be adequately resolved. There is a fundamental incompatibility between safeguarding principles and current practice concerning gender distressed children. Inherently, children are not adults. Schools should facilitate children to explore their ideas about themselves and the world in ways which do not harm them. While many schools believe they are acting in a child’s best interests, there is no circumstance in which safeguarding norms should be compromised. Nonetheless, this is happening across the country. The external political pressures on schools to adopt affirmative practice is driving them into making medical decisions they have no authority to make. Safeguarding measures protect both children and the staff who look after them. When safeguarding protocol is followed, schools do not overstep their role in a child’s life, and children do not suffer as a result.
| Recommendations
In line with mandatory safeguarding guidance and the law, parents should automatically be informed when a child discloses feelings of gender distress at school, unless there is a compelling reason for them not to be informed. Parents must be central to any further decision making regarding the handling of a child’s gender distress, including social transition or change of name. No school should facilitate a child’s social transition (the medical intervention in which a child adopts the social and cultural attributes associated with the opposite sex), unless medical advice clearly endorses this as the best and most appropriate action, and unless parents have been fully involved. Where this situation arises, schools should co-operate fully with relevant external agencies within their local authority. Schools should be required to publish all Relationships, Sex and Health Education (RSHE) material online, and have a clear process in place for parents to raise any concerns. Parents should be given an absolute right to see all RSHE materials their child will be taught at school. If it is not published online, it must be provided to parents on request, without any requirement for the parent to come on to the school premises. All agencies that provide materials to state-funded schools must accept that materials may be provided to parents in this way. The Government must urgently commission an indepent review of the teaching of RSHE materials and approach to gender distressed children in schools, with a focus on safeguarding. The review must be independent and not carried out by the Department for Education (DfE) which has been too closely involved in the development of the current situation. In line with the law and current guidance, certain activities and facilities should be single sex. This relates to toilets, changing rooms and sports of a competitive nature. There should be no exceptions to this. The DfE should update Keeping Children Safe in Education to explicitly address issues relating to children with gender distress and gender dysphoria, emphasising the importance of parental involvement in a child’s life. The document’s statement that LGBT is not a safeguarding issue needs to be removed, given the additional vulnerabilities of the current cohort presenting with gender distress. The Office for Standards in Education, Children’s Services and Skills (Ofsted) must routinely consider schools’ approach to gender-distressed children as part of its inspection of safeguarding protocols. A school’s failure to meet the appropriate standard should be reflected in the grade Ofsted awards the school, and treated with the same seriousness as other safeguarding failures. The DfE should issue guidance on what is not appropriate for schools to be teaching children in RSHE at different stages of a child’s education. Gender stereotypes must be effectively challenged in schools, without conflating beliefs about gender identity with sex. Discussion about gender-critical beliefs should be included. No state-funded school should subscribe to diversity membership schemes offered by external agencies where such organisations are involved in political campaigning. In accordance with the law, subscription to such schemes constitutes a fundamental conflict of interest. This does not prevent schools from purchasing or using external resources where no conflict arises. |