
Content
+
Foreword
Nimco Ali OBE
It has long been recognised that the safety, dignity and privacy of women and girls is improved when single-sex provision is available. Eradicating such provision is not progressive, nor is it justified, in a society where violence against one sex primarily by the other is the experience of millions of women and girls.
Eroding sexual boundaries does not erode the reality of biological sex and the oppression that comes with it. Health services that won’t guarantee intimate same-sex care or same-sex wards to vulnerable women will never stop women from needing these provisions. They just put women at a disadvantage, in the name of a misguided progression which is actually just a dressed-up form of 21st century misogyny.
The letter revealed by Policy Exchange in this paper marks yet another addition to a growing body of evidence which reveals the NHS to be seriously compromised by an ideology that is diminishing the rights of women and girls. Of course, transgender people also face a very real type of discrimination, and the law must protect them and enable them to live their lives freely. But when it comes to conflicting rights in a public institution like the NHS, decisions must be made with democratic consensus and full understanding that certain policies cannot be blindly endorsed simply because one minority is shouting the loudest for them.
There can be no compromise when it comes to women’s rights. There is no legitimate reason why a hospital cannot guarantee same-sex accommodation and intimate same-sex care, especially when the law explicitly allows for it. The right to privacy, dignity and safety as a patient is inextricably linked to the foundations of the NHS. To remove this right without consent is nothing short of a national scandal.
Next chapterKey points
- According to a letter seen by Policy Exchange, North Bristol NHS Trust (NBT) will not guarantee same-sex intimate care for patients, putting staff preferences above needs of patients. This is despite the trust’s biggest hospital recording up to 30 alleged incidences of sexual assault against females having taken place on hospital property.
- NBT refuses to ask its employees and staff members their biological sex, instead allowing them to self-identify their gender. This means an employee of the Trust who is biologically male but identifies as female is able to provide intimate care and clinical assistance to female patients.
- This Trust is unlikely to be unique. NBT’s policy on prioritising gender over biological sex is compatible with NHS same-sex accommodation guidance – which fails to understand the law and protect sex-based rights.
- The NHS is increasingly disregarding the realities and immutability of biological sex. It has strong links to lobbying group Stonewall, and senior NHS leaders have publicly endorsed gender identity ideology.
A letter from February 2021 written by North Bristol NHS Trust (NBT) contains policies that compromise the rights and legal protections applicable to female patients due to the policies being based on gender identity ideology. Both sex and gender reassignment are protected characteristics under the Equality Act 2010. This often results in a conflict between sex-based rights and the rights of transgender people (those who plan to undergo, are undergoing, or have undergone transition from their biological sex to a different gender).
The conflict between rights is not a new phenomenon. However, in a liberal democracy resolving such conflict should take place via democratic debate and consensus, transparency and backed by academic rigour. The prioritisation of gender above sex endorsed in this letter and by senior officials across NHS departments fundamentally falls to recognise the consequences of denying sex-based rights on patient safety, dignity and privacy.
Next chapterNHS Trust tells complainant they cannot guarantee intimate same-sex care from staff member
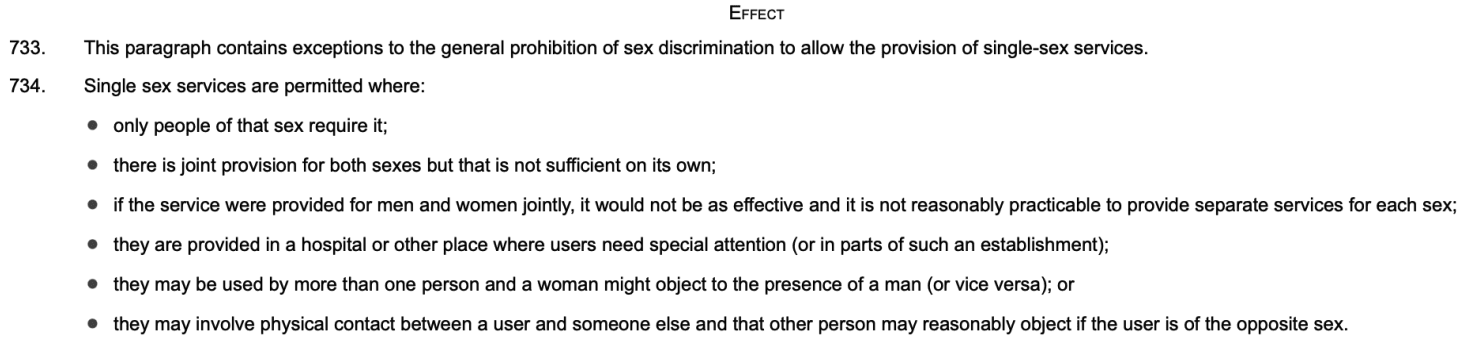
In a complaint response letter to a member of the public, former Chief Executive of NBT Evelyn Barker lays out policies that misinterpret sex and gender, and therefore explicitly disregard the need for same-sex accommodation and same-sex intimate care. The letter fails to take account of clear exceptions within the Equality Act 2010 which allow for same-sex intimate care and same-sex hospital wards:
‘Effect
-
- This paragraph contains exceptions to the general prohibition of sex discrimination to allow the provision of single-sex services.
- Single sex services are permitted where:
only people of that sex require it;
there is joint provision for both sexes but that is not sufficient on its own;
if the service were provided for men and women jointly, it would not be as effective and it is not reasonably practicable to provide separate services for each sex;
they are provided in a hospital or other place where users need special attention (or in parts of such an establishment);
they may be used by more than one person and a woman might object to the presence of a man (or vice versa); or
they may involve physical contact between a user and someone else and that other person may reasonably object if the user is of the opposite sex.’1Schedule (Three) 3, Part 7, Equality Act 2010, https://www.legislation.gov.uk/ukpga/2010/15/notes/division/3/16/20/7 (emphasis added)
Same-sex accommodation is compromised
The letter notes the complainant’s request to ‘take action and amend the policy to reflect that a male with male genitalia should not be able to access intimate spaces where women are undressed, drugged or sleeping.’
Despite initially confirming the policy of single-sex wards, the letter goes onto explain that in line with national guidance, wards are categorised by self-identified gender, making the concept of same-sex accommodation redundant.
‘These arrangements meet all national standards relating to single sex accommodation. ‘This includes allowing Trans people to be accommodated according to their presentation, the way they dress, and the name and pronouns they currently use. This may not always accord with the physical sex appearance of the chest or genitalia. Please refer to Annex B of the attached guidance from NHS: {Link to the policy}.’
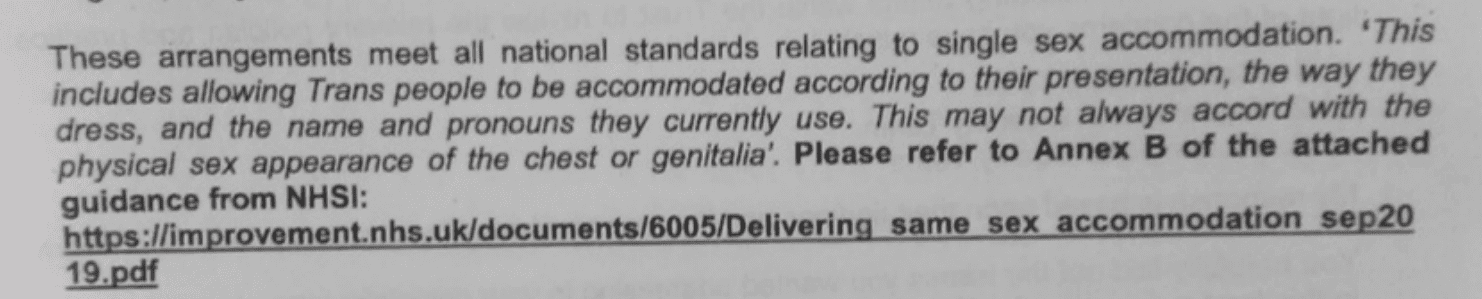
In practice, this means that a biological male will be accommodated with female patients on female wards (and vice versa) if requested by a patient who self-identifies as a gender not aligned to their biological sex.
This policy is enforced despite the allowances made under the Equality Act for single-sex provision where necessary.2Schedule (Three) 3, Part 7, Equality Act 2010, https://www.legislation.gov.uk/ukpga/2010/15/notes/division/3/16/20/7 As demonstrated below, the law itself explicitly states cervical cancer screenings and hospital accommodation as explicit examples of where same-sex provision is legitimate and lawful.
‘Examples
-
- These exceptions would allow:
a cervical cancer screening service to be provided to women only, as only women need the service;
a fathers’ support group to be set up by a private nursery as there is insufficient attendance by men at the parents’ group;
a domestic violence support unit to be set up by a local authority for women only but there is no men-only unit because of insufficient demand;
separate male and female wards to be provided in a hospital;
separate male and female changing rooms to be provided in a department store;
a massage service to be provided to women only by a female massage therapist with her own business operating in her clients’ homes because she would feel uncomfortable massaging men in that environment.’3Schedule (Three) 3, Part 7, Equality Act 2010, https://www.legislation.gov.uk/ukpga/2010/15/notes/division/3/16/20/7 (emphasis added)
Same-sex intimate care and patient consent is compromised
The letter goes on to reveal that the Trust cannot guarantee same-sex intimate care or gain full patient consent because it refuses to ask employees their biological sex.
‘there is no requirement for clinicians to disclose their gender identity. The Trust accepts that there may be some exceptions where a transgender person will be expected to disclose their gender identity such as where they are required to undertake personal care on vulnerable people. This statement will be rare and, where the staff member has their Gender Recognition Certificate and is fully transitioned to their preferred gender, this will not apply.’
While a clinician is expected to disclose where relevant their gender identity, the Trust confirms there is no policy requiring them to disclose their sex, and this expectation does not apply once a clinician has obtained a gender recognition certificate (GRC) and is ‘fully transitioned to their preferred gender’. The letter does not elucidate on what transition consists of.
The implications of this policy for patient consent are considerable. Under the Health and Social Care Act 2008, a clinician is legally required to gain the consent of the patient before they conduct any treatment, test or examination.4Section 2, Regulation 11, The Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, https://www.legislation.gov.uk/ukdsi/2014/9780111117613/regulation/11
Inextricably linked to whether a patient can give consent to have a particular treatment enacted upon them is the person in question enacting it. If a patient needed to have a particular surgery, they might consent to the surgery itself taking place, but would most likely remove this consent if they understood the surgeon proposing to perform the surgery was actually untrained.
The principle of intimate same-sex care rests upon the notion that a patient can consent to a treatment only when they know the sex of the clinician treating them. A person’s right to same-sex intimate care must be upheld for the sake of patient safety, dignity and privacy.
Same-sex intimate care is important, particularly for women who may have additional protected characteristics, such as religion or disability. For a woman who may be unable to defend herself against the biological strengths of a man, same-sex intimate care offers an additional level of safety and control to the patient, particularly if the patient is disabled or heavily medicated.
Intimate care can be distressing and naturally undignified, by virtue of the fact that a patient is entirely reliant upon their caregiver/clinician washing, touching or carrying out a procedure to intimate personal areas. For example, for a religious person whose beliefs might forbid the opposite sex from touching them in certain contexts, same-sex intimate care is an essential element to that patient’s privacy and dignity.
Similarly, in the context of women who are survivors of male sexual assault, the right to receive same-sex intimate care is essential to patient safety, privacy and dignity. Such situations are not hypothetical. Between 2015 and 2021, 17,195 women received NHS care in England because of assault. 7750 of these women were admitted to hospital and 476 of these episodes were caused by sexual assault.5NHS Digital, Admissions and finished consultant episodes for maltreatment and sexual assault, https://digital.nhs.uk/supplementary-information/2021/admissions-and-finished-consultant-episodes-for-maltreatment-and-sexual-assault Where women may be in hospital because of sexual assault, their sex-based right to intimate-same sex care is paramount.
Patient consent regarding same-sex intimate care relies on a patient knowing the biological sex of the person treating them. This is impossible if Trust staff are not required to disclose this where a concern may be raised.
Next chapterNorth Bristol NHS Trust’s sexual assault statistics reveal the importance of same-sex policies
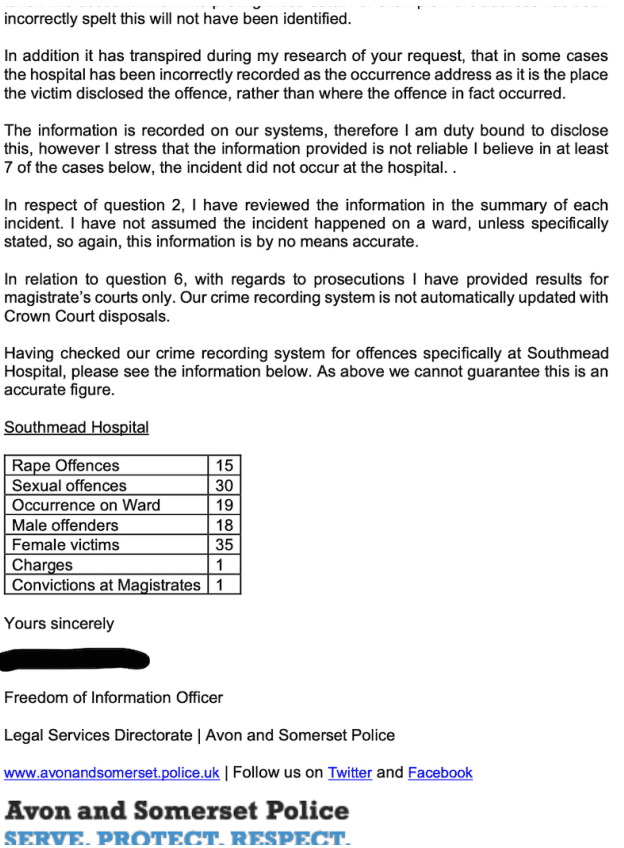
A recent FOI response reveals that since January 2019, up to 30 alleged sexual assaults have been committed against female patients at Southmead Hospital, the largest hospital under the provision of NBT.6Please refer to Annex A for the full FOI response.
| Rape Offences | 15 |
| Sexual offences | 30 |
| Occurrence on Ward | 19 |
| Male offenders | 18 |
| Female victims | 35 |
| Charges | 1 |
| Convictions at Magistrates | 1 |
It should be noted that this FOI response provided by Avon and Somerset Police contains some caveats. Notably, that regarding rape and sexual offences, ‘in some cases the hospital has been incorrectly recorded as the occurrence address as it is the place the victim disclosed the offence, rather than where the offence in fact occurred.’7The FOI also notes that its crime recording system is not automatically updated with Crown Court disposals, therefore the data provided here does not include the number of convictions in the Crown Court for more serious sexual offences, such as rape. The full FOI response can be found in the Annex A. However, the response does clarify that at least 19 occurrences definitely took place on hospital wards, as in these reports, the ward was explicitly stated as the location of the offence.8Please refer to Annex A for the full FOI response.
Regardless of where an assault takes place, it is clear that single-sex provision is a necessary sex-based right, both for those who may be in hospital because of an assault, those who have a history of being sexually assaulted and would accordingly find it distressing to receive intimate care from a biological male, and to attempt to prevent instances of assault occurring while a woman is in hospital.
Next chapterWider NHS guidance also compromises sex and gender
The misinterpretation of sex and gender in NBT’s policies are unlikely to be isolated, given national NHS guidance also fails to prioritise patient safety and privacy, as it dismisses sex-based rights in its 2019 same-sex accommodation policy Delivering same-sex accommodation.9NHS England and Improvement, Delivering same-sex accommodation, https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2021/05/NEW-Delivering_same_sex_accommodation_sep2019.pdf
‘Zero-tolerance approach’ has been compromised
In 2011, it became mandatory for NHS trusts to report monthly where they breached same-sex accommodation policies. This policy brought huge improvements in patient privacy and dignity. Between 2011 and 2019 (when the guidance was revised) the national breach rate dropped from 6.4 to 1.6.10The MSA breach rate is the number of MSA breachers per 1000 finished consultant episodes. Figures taken from January 2011 and January 2019, https://www.england.nhs.uk/statistics/statistical-work-areas/mixed-sex-accommodation/msa-data/
In 2019, despite reiterating its expectations for trusts to have a ‘zero-tolerance approach to mixed-sex accommodation,’ the revised guidance denies sex-based rights.
Consequently, it risks seriously compromising the advancements made for patient safety and dignity.111.2, Delivering same-sex accommodation
Annex B of the guidance compromises sex-based rights because it specifies that it is self-identified gender – not sex – that determines where transgender adults and ‘gender variant’ children should be accommodated.12Annex B, Delivering same-sex accommodation
The policy states:
‘A trans person does not need to have had, or be planning, any medical gender reassignment treatment to be protected under the Equality Act: it is enough if they are undergoing a personal process of changing gender.’13Ibid.
A biological male retaining his full physiological makeup, and who does not plan to acquire a gender recognition certificate (GRC) or undergo surgery, can self-identify as female and be accommodated on a female ward. Further, a person does not need to live continuously in their new gender in order to access the accommodation of the opposite sex. They simply need to be going through ‘a personal process of changing gender’ to be accommodated in an opposite sex ward.14Ibid.
As demonstrated above, the Equality Act 2010 specifically references same-sex hospital wards as a legitimate reason to discriminate on the basis of sex.
While acknowledging this exemption, the guidance stipulates that it will consider it only on a ‘case-by-case basis’, by assessing the detriment to the transgender person if they are refused admission or the detriment to the other service users if the transgender person were to be allowed access. The guidance states:
‘There may be some circumstances where it is lawful to provide a different service or exclude a trans person from a single sex ward of their preferred gender but only if this is a proportionate means of achieving a legitimate aim. Any decision to do this must therefore be made on a case-by-case basis, and based on:
- an objective and evidence-based assessment of the circumstances and relevant information
- respecting the rights and needs of the trans person and the detriment to them if they are denied access and balancing that against the needs of other service users and any detriment to them if the trans person is admitted.’15Ibid.
Despite the Equality Act’s explicit provision for single-sex provision, NHS guidance deploys this exemption as an exception, not a rule.
NHS guidance is therefore clear that trusts are not obliged to offer same-sex accommodation. It follows that the monthly data collection by trusts on breaches of the same-sex accommodation policy mandated by NHSE is actually collected by gender, not sex. This national guidance remains in application.
Next chapterGender identity ideology is compromising patient safety and dignity across the NHS
The NHS is increasingly becoming influenced by gender identity ideology, which disregards the realities and immutability of biological sex. This is being done in the absence of democratic consensus and with very little understanding for the consequences for patient safety and rights, particularly the rights of women and children.
Senior leaders within the NHS neglecting sex-based rights
In November 2022, Dr Navina Evans, Chief Executive of Health Education England (HEE), committed the organisation to ‘to become active trans and non-binary allies.’16The full statement can be read in Annex B.
The statement references ‘the public debate’ around trans rights, but proceeds to ‘ally’ itself to just one side of it:
‘In recent months, the public debate around trans and non-binary rights has intensified. As HEE’s leadership, we have growing concerns about the hostility that trans and non-binary staff & patients are experiencing.’
‘Now, more than ever, is the time to educate ourselves and others to become active trans and non-binary allies. Within HEE, we have been making consistent efforts to understand and appreciate the experience of our trans and non-binary colleagues. We are having conversations, developing our own understanding, and continuing our learning. We have made progress, but we have a long way to go on our journey. We are confident that this is the only right way forward that reflects our values and the values of the wider NHS.’
Discrimination and hostility towards transgender people is of course unacceptable and should not be tolerated. However this statement shows a distinct lack of awareness of a much wider issue; that incautious ‘allyship’ towards transgender rights risks compromising sex-based rights. As a public institution that is supposed to be politically neutral, this statement takes a distinct position on a contentious political issue.
LGBT+ lobbying group Stonewall is explicitly endorsed by Evans in this statement, despite Stonewall’s track record of lobbying for the Gender Recognition Act 2004 to be reformed to enable self-ID to become the law.17Stonewall, Stonewall statement on Gender Recognition Act reform, https://www.stonewall.org.uk/about-us/news/stonewall-statement-gender-recognition-act-reform
Links to lobbying groups at different levels across NHS departments
Stonewall has strong links to the NHS. HEE received a ‘gold’ award from Stonewall in February 2022, coming 110th out of 403 employers in Stonewall’s Workplace Equality Index (WEI), marketed as the charity’s ‘definitive benchmarking tool for employers to measure their progress on lesbian, gay, bi and trans inclusion in the workplace.’18Stonewall, Stonewall UK Workplace Equality Index, https://www.stonewall.org.uk/creating-inclusive-workplaces/workplace-equality-indices/uk-workplace-equality-index
Of 100 ‘top employers’ four NHS trusts, NHS Business Services Authority and NHS England and Improvement (NHSE&I) featured in 2022.
In its 2022 WEI Employer Feedback Report to NHSE&I, Stonewall commented on NHS policies and procedures, noting that asking trans employees for their GRC when updating staff information ‘may create unnecessary barriers for them to have their identities recognised’.19Stonewall Workplace Equality Index 2022: Employer Feedback Report, https://www.whatdotheyknow.com/request/883161/response/2160412/attach/7/2208%201809495%20Q5%20Feedback%20Received%202022.pdf?cookie_passthrough=1
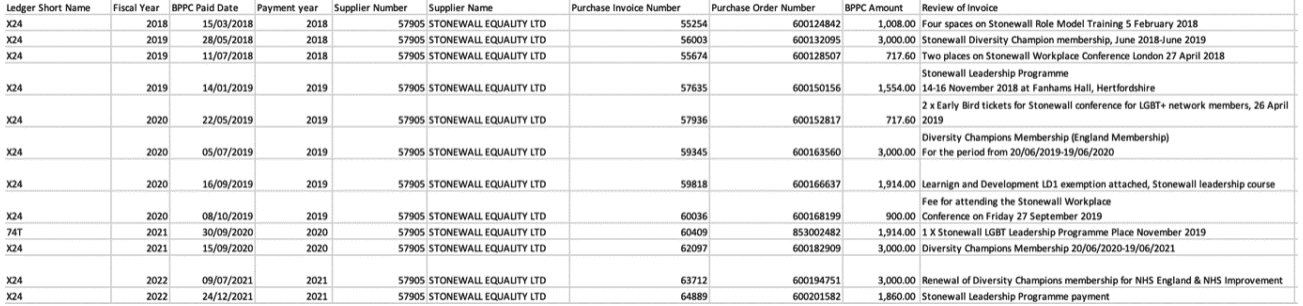
An FOI request response from July 2022 states that NHS England has applied to Stonewall’s WEI for the last four years and has paid over £22,000 in membership fees, training course costs and conferences since 2018.20FOI Request: Stonewall Workplace Equality Index scheme (WEI), https://www.whatdotheyknow.com/request/stonewall_workplace_equality_ind_2#incoming-2160275
Recommendations
- North Bristol NHS Trust and all other NHS trusts must uphold a patient’s right to same-sex intimate care and same-sex accommodation on hospital premises.
- NHS England & Improvement should revise ‘Delivering same-sex accommodation’ to remove Annex B, and state clearly that sex does not mean gender, but biological sex.
- NHS England, all NHS Trusts and all other public bodies associated with the NHS should withdraw from membership of actively political or lobbying organisations such as Stonewall.
Annex A
Legal Services Directorate
Force Headquarters, PO Box 37, Valley Road,
Portishead, Bristol, BS20 8QJ
Email foirequests@avonandsomerset.police.uk
| Name Redacted
Email redacted |
Our Reference | 968/22 |
| Date | 27 September 2022 |
Dear (Name Redacted)
I write in connection with your request for information dated 26th August under the Freedom of Information Act.
Specifically you asked:
- Since 1 January 2019, how many reports were made to the police of incidents at Southmead Hospital of (a) alleged rape and (b) alleged sexual assault excluding rape?
- How many of these reported incidents took place on hospital wards?
- How many of the alleged perpetrators were biologically male?
- How many of the alleged victims were biologically female?
- How many people have been charged as a result of these reports?
- How many successful prosecutions have been brought as a result of these reports?
Our response:
You have requested all reported offences that occurred at this specific location. The offences captured by this request relate to for example, indecent exposure, sexual assault by touching, and rape allegations. This of course relates not only to reports made by patients, but also reports by staff.
The detail collected to respond specifically to your request is subject to the inaccuracies inherent in any large scale recording system. As a consequence, care should be taken to ensure data collection processes and their inevitable limitations are taken into account when interpreting those data. For example if the address has been incorrectly spelt this will not have been identified.
In addition it has transpired during my research of your request, that in some cases the hospital has been incorrectly recorded as the occurrence address as it is the place the victim disclosed the offence, rather than where the offence in fact occurred.
The information is recorded on our systems, therefore I am duty bound to disclose this, however I stress that the information provided is not reliable I believe in at least 7 of the cases below, the incident did not occur at the hospital.
In respect of question 2, I have reviewed the information in the summary of each incident. I have not assumed the incident happened on a ward, unless specifically stated, so again, this information is by no means accurate.
In relation to question 6, with regards to prosecutions I have provided results for magistrate’s courts only. Our crime recording system is not automatically updated with Crown Court disposals.
Having checked our crime recording system for offences specifically at Southmead Hospital, please see the information below. As above we cannot guarantee this is an accurate figure.
Southmead Hospital
| Rape Offences | 15 |
| Sexual offences | 30 |
| Occurrence on Ward | 19 |
| Male offenders | 18 |
| Female victims | 35 |
| Charges | 1 |
| Convictions at Magistrates | 1 |
Yours sincerely
Name Redacted
Freedom of Information Officer
Legal Services Directorate | Avon and Somerset Police
www.avonandsomerset.police.uk | Follow us on Twitter and Facebook
Annex B
Health Education England statement of intent, publicly committing to trans inclusion and equality in support of the trans and non-binary community.
14 November 2022
Dr Navina Evans, Chief Executive, Health Education England commits Health Education England to the below statement of intent:
All human rights are compromised if any one group is excluded. We are at our best when we stand together, and we all have a role in ensuring our NHS is a place where all our citizens are treated with respect, dignity, and compassion.
In recent months, the public debate around trans and non-binary rights has intensified. As HEE’s leadership, we have growing concerns about the hostility that trans and non-binary staff & patients are experiencing.
A fundamental promise of the NHS is that we exist for all and we have a duty of care to all. It is crucial that everyone, including trans and non-binary people, feel respected, safe and receive an equal level of care. As a healthcare organisation we want to reiterate our commitment to implementing the spirit and the letter of the Equality Act – by striving to create an NHS that is fair and truly inclusive.
Diversity and inclusion is of great importance to us, not only morally, but also in a business sense, because inequalities in healthcare organisations are likely to be reflected in our work and adversely impact the populations we serve. Being inclusive is essential to enabling us to attract the best talent and provide the best possible care for the people we serve – our patients.
LGBTQI+ charities and the organisations that support them have also seen increased hostility, with much of it focused on the Stonewall Diversity Champions Programme. Many organisations in health and care have found Stonewall helpful as a way of developing a sense of belonging and inclusion for LGBTQI+ staff, and in HEE we welcome the support Stonewall provides us to help achieve this aim.
Now, more than ever, is the time to educate ourselves and others to become active trans and non-binary allies. Within HEE, we have been making consistent efforts to understand and appreciate the experience of our trans and non-binary colleagues. We are having conversations, developing our own understanding, and continuing our learning. We have made progress, but we have a long way to go on our journey. We are confident that this is the only right way forward that reflects our values and the values of the wider NHS.
We stand with the trans and non-binary community.